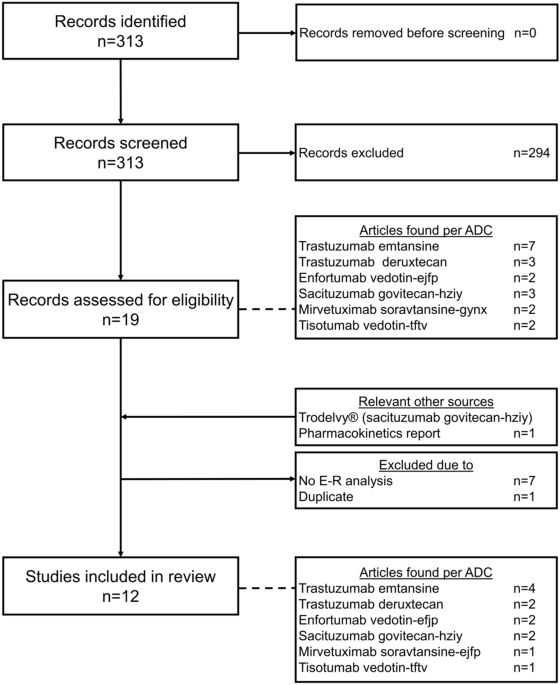
In this review, popPK and popPD studies of therapeutic enzyme therapy in LSDs were summarized. Six popPK studies covering four different LSDs were selected [21,22,23,24,25,26], two of which also contained popPD analyses [23, 25], and one study investigated exposure-response relationships [29]. From all available popPK analyses, four studies also included data from pediatric patients.
As summarized in Table 1, all included studies included fewer than 100 subjects and relied on data obtained from Phase I/II and Phase III clinical trials, which inherently limit IIV and the ability to robustly characterize exposure-response relationships. Nevertheless, the majority of studies employed extensive plasma sampling schemes, with at least 8 samples and up to 31 samples per subject, enabling reliable popPK model development. Furthermore, all studies included in this review applied the NLME modeling approach for the analysis of PK and PD data. Nonlinear mixed-effects modeling is widely regarded as the gold standard in popPK/PD analyses, as it allows for the characterization of both PK/PD parameters in the population, quantification of variability between and within patients, and identification of covariates explaining the variability in PK/PD parameters [13, 30, 31]. The advantage of NLME modeling is its ability to reliably obtain PK and PD models using sparse clinical data, which is particularly relevant in rare diseases such as LSDs, where patient numbers are limited and rich sampling is often not feasible or unethical (e.g., pediatric patients) [30]. The NLME modeling approach is also used in simulating alternative dosing regimens, which can support dose optimization and trial design. Nevertheless, one should not forget that NLME modeling requires assumptions about structural and statistical models, which may influence parameter estimates and predictions. Model evaluation and external validation are, therefore, critical steps to ensure robustness of the model and reliability of the results.
The estimated Vcs reported by Qi et al. (1.52 L) and Gras-Colomer et al. (1.10 × 10−2 L in plasma and 2.57 × 10−1 L in leukocytes) are markedly low, particularly when compared with the values reported in the other included studies (approximately 3.5 L). Qi et al. determined the Vc for an MPS VII subject with a baseline body weight of 20 kg [23]. The predicted apparent Vc of 1.52 L in a 20 kg pediatric patient corresponds to approximately 76 mL/kg, which is within the expected range of blood volume in children. For a large hydrophilic enzyme such as vestronidase alfa, largely confined to the intravascular and extracellular space, this estimate is pharmacokinetically plausible. Gras-Colomer et al., on the other hand, suggest in their discussion that the low predicted apparent Vc values could reflect a high distribution into target organs, where leukocytes are transformed into tissue macrophages [25]. They further note that the volume of distribution of peptides is generally small and limited to the extracellular space, which is consistent with the findings of the present analysis. Despite this explanation, these values seem unrealistically small.
In four popPK studies, the occurrence of ADAs was assessed as a covariate for explaining IIV in estimated PK parameters [21,22,23, 26]. The impact was considered typically through graphical evaluation of ADA titers and neutralizing activity in relation to drug concentration. In some cases, high ADA titers were associated with reduced systemic concentrations of the therapeutic enzyme, and neutralizing ADAs corresponded with concentrations below the limit of quantification, suggesting a potential influence on drug disposition. However, the presence of ADAs was not included as a covariate in the final popPK models, often due to small sample sizes, sparse ADA data, or lack of consistent trends across patients. Anti-drug antibodies can alter pharmacokinetics by increasing clearance, formation of immune complexes, or neutralizing drug activity, which may diminish exposure and thus efficacy [9, 10]. In LSDs specifically, immunogenicity to ERT frequently occurs, particularly in patients lacking residual endogenous enzyme activity [32]. Although the impact of ADAs is often explored descriptively, for example, by comparing individual PK parameters or exposure metrics according to ADA status, their effects are rarely quantified within popPK/PD models. This is likely due to limited sample sizes, sparse longitudinal ADA data, and uncertainty regarding neutralizing capacity. While incorporating ADA measurements as time-varying covariates could improve characterization of exposure-response relationships, practical implementation is often challenging given the constraints of typical clinical trial datasets in rare diseases.
In three of the included studies, allometric scaling was applied to scale the population PK parameters [22, 23, 26]. Allometric scaling is a widely used method that provides a simple and empirical approach for extrapolating PK parameters from adults to pediatric patients by accounting for differences in body weight in drug disposition. Clearance is commonly scaled to body weight using an exponent of 0.75, while volume of distribution is scaled with an exponent of 1.0, reflecting established physiological principles across species and age groups. However, these fixed exponents may not always hold in pediatrics, particularly in neonates and infants, as maturation of metabolic pathways, organ function, and drug-specific properties contribute substantially to clearance and volume of distribution beyond body weight alone [33, 34]. In one study, a time-varying value for body weight was considered for the allometric scaling process since the body weight of the pediatric population increased during the clinical study [22]. Troy et al. developed a two-compartment model for CSF data and a one-compartment model for plasma data. Weight-based allometric scaling was applied to the systemic components of the model, whereas a non-allometric age-based scaling method was used for the brain components to improve model fit, since brain maturation correlates more reliably with age than with TBW in children with MLD [26]. The studies included in this review identify TBW as a significant covariate for both CL and Vc. These findings suggest that the distribution and elimination of ERTs are influenced by TBW and may also be affected by body composition, underscoring the importance of body weight as an explanatory factor for IIV in CL and Vc in patients treated with ERT. As ERTs comprise large, hydrophilic proteins administered IV, their distribution is largely confined to the vascular and interstitial spaces. Therefore, IIV associated with their population PK parameters may be more correlated to LBW or IBW than to TBW. However, this has not been studied to date. Therefore, we would like to emphasize the importance of evaluating additional morphometric parameters beyond TBW. Dosing based solely on TBW may result in relatively high exposure in individuals with a high body fat percentage (high body mass index), in case that Vc and CL scale with morphometric parameters other than TBW.
The pharmacokinetics of therapeutic enzymes are often nonlinear, and extensive mathematical modeling may be required for resolving complexities associated with their disposition [35]. Therapeutic enzymes are cleared from the bloodstream via both receptor-mediated processes, such as mannose 6-phosphate (M6P) receptor-mediated endocytosis, and non–receptor-mediated pathways, including non-specific proteolytic degradation [57, 58]. At lower concentrations, clearance can be rapid due to high receptor affinity, whereas at higher concentrations these receptors may become saturated, leading to a nonlinear relationship between dose and systemic exposure, as reported in the study conducted by Qi et al. [23]. Tuffal et al. observed a transient saturation of the nonlinear (Michaelis–Menten) clearance pathway during the infusion period of avalglucosidase alfa, when plasma concentrations were increasing toward Cmax [21]. Since this saturable process was limited to the high plasma concentrations achieved during infusion, the duration of saturation was prolonged at higher dose levels. However, Michaelis–Menten clearance contributed minimally to overall systemic clearance. While nonlinear clearance is usually saturated at concentrations above Km, simulations demonstrated that linear clearance predominated across the plasma concentration range observed at the approved dose of 20 mg/kg every 2 weeks. Overall, saturable uptake contributes to variability in drug disposition across patients, especially when variability in receptor expression, disease severity, or body weight affects enzyme distribution and clearance [58]. In a popPK analysis, these processes can be characterized and applied to guide dose optimization and individualization [22]. However, in popPK analyses, drug disposition is primarily data-driven and does not take the full physiological information into account. To evaluate and predict the potential efficacy of ERT in LSDs, there is a need to understand the physiological distribution of the drug and variables that may affect this. In contrast, physiologically based pharmacokinetic (PBPK) modeling provides a mechanistic approach to understand how drug properties and physiological processes affect pharmacokinetics. Physiologically based pharmacokinetic models make use of a larger number of compartments, each representing different organs and tissues connected by the circulatory system. This approach incorporates detailed physiological parameters, such as organ blood flow and tissue composition, allowing for better extrapolation across populations or species. While PBPK modeling can be used to estimate common PK parameters, it is particularly valuable for understanding drug behavior at a specific tissue level, which popPK cannot fully capture mechanistically [36]. The PBPK of therapeutic enzymes enables prediction of tissue concentration profiles that are relevant for analyzing on-target PD effects [37,38,39]. Despite its potential to capture complex processes such as tissue distribution, PBPK modeling remains largely unexplored for therapeutic enzymes in LSDs, with only a few exploratory studies reported to date [4, 40]. This represents an important opportunity for future research, as this approach could provide added value in optimizing dosing strategies for ERT in LSDs, where the most appropriate dosage regimen remains controversial.
The effectiveness of ERT is strongly influenced by enzyme half-life, which differs markedly between plasma and intracellular compartments. Following IV administration, therapeutic enzymes circulate in plasma, where they typically exhibit short half-lives (minutes to 2.5 h). This is largely due to rapid receptor-mediated uptake, primarily via the M6P receptor. Consequently, plasma exposure declines rapidly after infusion. For ERT to be effective, the enzyme must be internalized by target cells and trafficked to lysosomes, where a prolonged half-life (between 2 and 9 days) allows sustained enzymatic activity. These contrasting half-lives have important therapeutic implications. While the short plasma half-life limits circulating enzyme availability, intracellular persistence largely determines the duration of the PD effect and clinical benefit. This distinction helps to explain why many ERTs are administered intermittently, despite rapid plasma clearance. For most ERTs, intracellular half-lives are sufficiently prolonged to support dosing intervals of 1–2 weeks or longer rather than daily administration.
Despite their short plasma half-life, most therapeutic enzymes demonstrate clinical efficacy that extends well beyond baseline levels [41]. This demonstrates that intracellular and plasma PK might differ. In two studies, the intracellular PK was evaluated in plasma leukocytes and monocytes. In LSDs, therapeutic enzymes are predominantly internalized by receptor-mediated endocytosis into target cells. Moreover, the extent of this cellular uptake is a key determinant of ERT efficacy. In contrast, plasma concentrations of therapeutic enzymes decline quickly due to the short half-life of the enzymes and rapid tissue distribution. Thus, serum PK profiles primarily reflect distribution and clearance rather than intracellular availability. It is hypothesized that cellular enzyme activity correlates better with substrate reduction and clinical improvement than serum enzyme activity [24]. Leukocytes can be readily obtained from blood and are an accessible surrogate for leukocytes residing in tissue [24, 25]. Consistent with that, Gras-Colomer et al. developed a popPK/PD model in GD that linked leukocyte GCase activity to improvement in bone-marrow infiltration by macrophages (Gaucher cells), an important parameter for evaluating disease severity [25]. In this analysis, intracellular exposure is supposed to best predict clinical response, underscoring intracellular PK as the relevant exposure metric for ERT. These findings support using leukocyte enzyme activity to guide dose optimization and individualization. Accordingly, intracellular PK may better reflect actual PD effect and could be more relevant for understanding ERT responses [42]. Intracellular enzymatic activity is considered a PK endpoint for predicting individual enzymatic activity [25]. Therefore, intra-leukocyte activity is a possible marker for therapeutic individualization in patients receiving ERT in LSDs [43]. However, it is important to note that Qi et al. successfully developed a popPK/PD model for vestronidase alfa based on plasma concentrations, demonstrating that systemic PK parameters can also adequately describe exposure-response relationships in LSDs [23].
In the study by Troy et al., the PK of a therapeutic enzyme in CSF was evaluated [26]. Intravenously administered enzymes are not expected to cross the blood–brain barrier (BBB) [44, 45], whereas the majority of LSDs affect the brain [44]. Therefore, targeting the CNS in LSDs remains a major challenge. Beyond dose adjustments and alternative routes of administration, enzyme modifications such as fusion proteins and chemical changes that alter receptor affinity can increase blood concentrations of therapeutic enzymes and help maintain higher levels at the BBB for a prolonged period [46, 47]. Recently, Muenzer et al. reported the first results of a Phase 1–2, open-label study evaluating the safety and efficacy of tividenofusp alfa in children with MPS type II (MPS II) [59]. Tividenofusp alfa, a novel fusion protein using the transferrin receptor to cross the BBB, is administered IV while targeting the CNS. However, plasma PK provides limited insight into drug exposure at the intended site of action. Characterization of PK in CSF, and ideally in brain tissue, may offer more meaningful information on enzyme distribution, persistence, and pharmacologically relevant concentrations in the target organ. The popPK analysis of intrathecal-administered arylsulfatase A in patients with MLD by Troy et al., illustrates this principle: CSF concentrations were described by a two-compartment CNS model with rapid distribution into a brain tissue compartment and a remarkably long terminal half-life in the CNS (ca. 480 h), suggesting sustained drug persistence in the brain between two doses. These findings underscore the importance of assessing tissue concentration rather than relying solely on plasma exposure to link enzyme disposition to clinical outcomes and to guide optimization of dosing strategies.
The relationship between the PK of therapeutic enzymes and their efficacy in patients with LSDs has hardly been investigated despite it being an important step for evaluating and predicting treatment outcomes. Linking PD data to the existing popPK model provides a more robust framework for predicting both enzyme exposure and its corresponding therapeutic effects, enhancing the clinical relevance of the model [48]. A popPK/PD model for therapeutic enzymes would provide insights into the concentration-effect relationship, allowing for a deeper understanding of how enzyme concentrations correlate with clinical efficacy and safety outcomes in patients with LSDs. Furthermore, such a model may support individualized dosing strategies, optimizing therapeutic outcomes by accounting for both IIV in drug exposure and its corresponding PD response. This also highlights the potential importance of intracellular drug concentrations in determining efficacy and in understanding and predicting inter-subject variability in drug response. Berger et al. selected intracellular concentrations for the development of a popPK model for imiglucerase based on the observation that the biweekly dosing regimen does not correspond with the very short plasma half-life of imiglucerase of just a few minutes. In the absence of pharmacological evidence to explain the clinical efficacy of this regimen, they hypothesized that intracellular PK may be more relevant than plasma PK for understanding ERT response. Given this apparent paradox between the very short plasma half-life and the clinical efficacy of imiglucerase, they proposed that intracellular and plasma PK might differ [24]. Similarly, Gras-Colomer et al. developed a popPK model incorporating both plasma and leukocyte enzymatic activities. For the exposure-response analysis, leukocyte enzymatic activity was selected, given that the monocyte/macrophage system represents the primary target in GD1. In addition, plasma enzymatic activity has shown higher IIV than leukocyte enzymatic activity, possibly due to the short plasma half-life of the therapeutic enzyme [25]. However, quantifying intracellular drug concentrations directly in humans is challenging. In the included studies intracellular concentration was assessed using circulating plasma monocytes and leukocytes. In GD1, uptake of imiglucerase via the mannose receptor on circulating blood monocytes has been shown to serve as an accessible surrogate for tissue macrophages [54, 55]. Moreover, pharmacokinetic-biomarker analyses based on GCase activity in leukocytes have demonstrated a good correlation with clinical response to ERT [53, 56]. However, in a previous study, Gras-Colomer et al. carried out an analysis using samples containing proportions of different leukocyte subsets [53], while enzyme activity has been shown to be 40- to 50-times higher in monocytes compared with lymphocytes and neutrophils in patients with GD1 [54]. In Pompe disease, the primary target tissues of recombinant human acid alpha-glucosidase (rhGAA) are cardiac and skeletal muscles, where the enzyme is transported to lysosomes to break down glycogen. Plasma drug concentrations are often used as a surrogate for tissue exposure, based on the assumption that systemic drug concentrations reflect intracellular drug concentrations at the site of action. However, previous research in Fabry and Pompe disease has demonstrated that this assumption does not fully apply to alglucosidase alfa and agalsidase beta and is likely also not applicable to other ERTs internalized via the M6P receptor due to the so-called 'sink effect' [49]. High expression of M6P and mannose receptors in organs like the liver and spleen causes significant uptake of the enzyme early after infusion, preventing it from reaching the main target tissues and thus acting as a sink. In GD, this phenomenon is advantageous as the macrophages in the liver and spleen are the target tissues. In the less favorable cases, increasing the enzyme dose may help to overcome this effect, although it may also increase the risk of adverse effects or antibody formation [50]. Further research on intracellular exposure is essential to determine therapeutic efficacy and to improve the understanding and prediction of IIV in ERT response.
Among the included studies, only a few popPD analyses have been published whereas popPK analyses are more abundant. In the study from Qi et al., an indirect response model linking vestronidase alfa exposure to reduction in urinary glycosaminoglycans (uGAGs) in patients with MPS was established [23], whereas Gras-Colomer et al. applied a discrete-time Markov model to capture the relationship between predicted imiglucerase exposure in leukocytes and the probability of transition between different stages of bone marrow infiltration by Gaucher cells in GD [25]. In contrast, all other studies focused primarily on PK characterization, with PD evaluation limited to exploratory exposure-response analysis [


Comments (0)