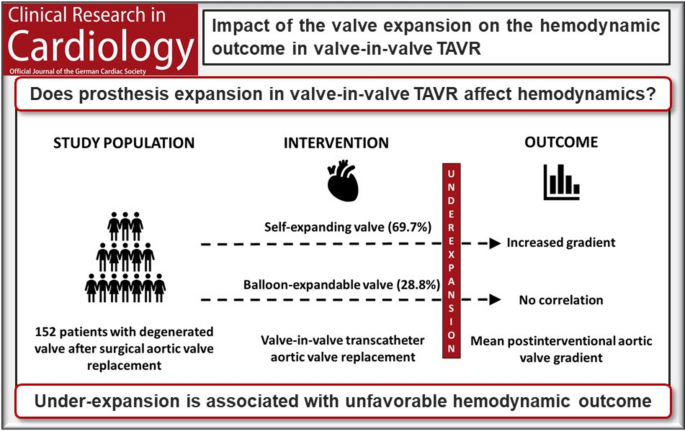
In this study, we analyzed the periinterventional prosthesis expansion and implantation depth and the association with the hemodynamic outcome in valve-in-valve TAVR. Until now, our cohort is the largest of comparable studies. We propose a new expansion ratio threshold which correlates with the hemodynamic outcome in SE valves. After normalization to the expected gradient, we still observed a correlation with the waist expansion. Consequently, we assumed that the correlation between under-expansion and the hemodynamic outcome is independent of the valve type and size in SE valves. Surprisingly, no effect was found in BE valves. The reasons remain unclear; it might be possible that the cohort size was too small to identify a significant difference in the BE group. In our cohort, a relatively high number of patients were diagnosed with an elevated pmean of at least 20 mmHg after intervention. This might be caused by the small mean anulus and true inner diameter of the initial surgical valve prostheses. We found no significant association between pmean and true inner diameter, possibly due to the small number of patients in the subgroups. Patient-prosthesis mismatch might have an influence on the hemodynamic performance of the TAVR prosthesis. Yet, a consistent and clinically relevant correlation could not be observed in our cohort, possibly due to the heterogenicity of the prosthesis combinations.
We observed that in our cohort, post-dilation was a successful tool to improve the waist expansion. Yet, it must be taken into consideration that post-dilation in our cohort was not only performed due to under-expansion, but also due to paravalvular leakage in some patients. A recent study could show a favorable effect of post-dilation on the hemodynamic outcome in valve-in-valve TAVR in a comparable collective [19]. The authors observed reduced postinterventional gradients in patients who received a post-dilation of SE valves. However, no periinterventional measurement was performed to assess the effect of post-dilation on the waist expansion. Further, our results are congruent with a study performed by Fukui et al. in 2023 [20]. The research group examined 53 patients who received a valve-in-valve TAVR with SE prostheses and analyzed the computed tomography scans 30 days after intervention. They observed a correlation between under-expansion of the waist and increased postinterventional gradients. However, no periinterventional angiographic expansion measurement or analysis of post-dilation was performed.
Our data suggest that an angiographic periinterventional measurement of the waist in valve-in-valve TAVR might be a valuable tool to recognize under-expansion at a point in time when it is still possible to react immediately to it. Especially in SE valve prostheses, a post-dilation might be considered in case of a relevant under-expansion to improve the hemodynamic result. In addition, periinterventional measurement might help to prevent unnecessary dilation with the potential risk of stroke, valve damage, or annulus rupture [12, 21]. Yet, the effect needs to be proven in a prospective study.
Another option to improve the valve expansion is the bioprosthetic valve fracture [22, 23]. Valve fracture gives the opportunity to enlarge the annulus diameter and prevent under-expansion and patient-prosthesis mismatch, but a higher risk of bleeding and mortality has been reported [24]. In our cohort, no valve fracture was performed, as it was not part of the standard procedure in our clinic. Yet, a small retrospective study showed a favorable effect of bioprosthetic valve fracture on the postinterventional mean gradient [25]. Future prospective studies will be necessary to assess potential effects on the hemodynamic outcome.
Moreover, we observed that increased postinterventional gradients after valve-in-valve TAVR are associated with a deep implantation of the prosthesis. These results are in line with previous studies [16, 20, 26]. Until now, the exact mechanism remains unclear. We observed a correlation between implantation depth and waist expansion, so one might hypothesize that the deep implantation prevents an optimal valve expansion within the waist area. Taken together, the data suggest that a high implantation of SE valves should be preferred. However, a higher implantation can increase the risk of a coronary obstruction [27, 28]. Finally, the effect of implantation height should also be analyzed in larger studies with detailed hemodynamic assessment.
It needs to be mentioned that only a few data about the impact of elevated postinterventional gradients on the long-term outcome of valve-in-valve TAVR exist. The FRANCE-2 registry could show a higher mortality of patients with elevated gradients after native TAVR [29]. The PARTNER-2 registry found a correlation between elevated gradients and increased mortality 1 year after valve-in-valve TAVR8. Yet, another study by Alperi et al. found no significant correlation between postinterventional gradients and mortality [30]. More long-term follow-up data will be necessary for the assessment of this effect.
Limitations
This was a retrospective observational study, and different types of bias can therefore not be ruled out. Moreover, only patients from two hospitals were included, which means that local standards and workflows may limit the generalizability of these results. The number of patients enabled reliable statistics but may have been underpowered to allow significant differences in subgroup analyses. Due to the different implantation mechanism, patients who were treated with TAVR-in-TAVR were not included in this analysis. Since, in the routine TAVR procedure, the expansion of the prosthesis is only visualized fluoroscopically in one plane, the analyses of the expansion could also only refer to this single plane. Due to the circular structure of the initial SAVR prostheses, however, it seems reasonable to expect an approximately symmetrical expansion. Yet, in a further study, a validation of the valve expansion, for example, in a postinterventional computed tomography, should be performed. As we included all suitable cases in this retrospective study, standardized follow-up data were not available. Future prospective studies will be necessary to assess the clinical impact of our observations. Furthermore, due to the design, the results of this study are only suitable for generating hypotheses and should not cause clinical implications.


Comments (0)