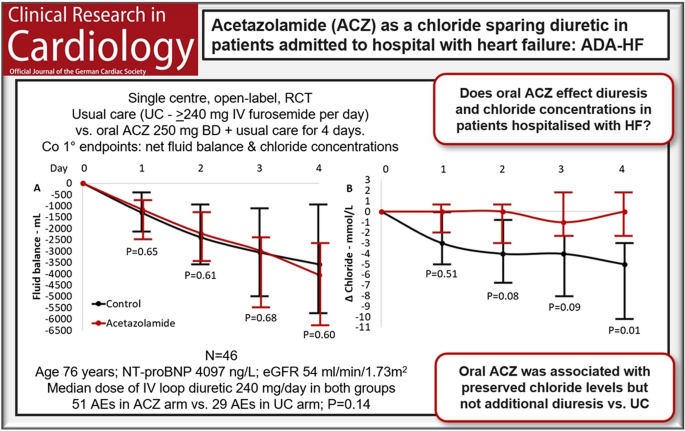
Our pilot study suggests that oral acetazolamide 250 mg twice a day may protect against chloride loss during treatment with a high-dose IV loop diuretic but may not have much diuretic effect compared to a high-dose loop diuretic alone.
Acetazolamide and diuresis
The ADVOR trial found that over three days, 500 mg of IV acetazolamide alongside low-dose IV furosemide compared to low-dose IV furosemide alone was associated with a greater diuresis (by 500 mL) and a greater natriuresis (by 98 mmol) after 48 h of treatment. The study was formally positive: acetazolamide was associated with a 46% greater chance of achieving euvolaemia after 48 h compared to placebo, with a number-needed-to-treat of 6 [8].
However, the study used IV acetazolamide, which is sometimes difficult to access, and only a low-dose loop diuretic as a comparator. Whether oral acetazolamide has any effect when added to high-dose IV furosemide is not known.
It is traditionally taught that mucosal oedema in the gastrointestinal tract reduces drug absorption in patients with congestion, but there is no difference in the diuretic or biochemical effect between IV and oral administration of adjunctive diuretics such as thiazide diuretics [13], or tolvaptan [12]. Acetazolamide appears to follow the same rule: although oral ACZ had no diuretic effect, we found that, like IV acetazolamide [13], it does affect serum and urine electrolytes, so it must be being absorbed [14].
Although our study was underpowered to detect modest differences, we found no statistically significant difference in diuresis. Similarly, the DEA-HF trial also found no additional diuresis with IV acetazolamide (one dose of 500 mg IV) in addition to high-dose IV furosemide (one dose of 250 mg IV) compared to IV furosemide alone in ambulatory patients with HF [15].
In the DOSE trial, high-dose furosemide (~ 260 mg per day) was superior to low-dose (~ 120 mg per day) for diuresis and improving symptoms of breathlessness [16]: the high-dose loop diuretic should be the comparator for any trial of combination diuretic therapy [17].
Most patients are admitted to hospital with HF with many litres of excess fluid1[1, 18], so although the difference in diuresis after 3 days found in ADVOR was statistically significant, it took a trial of 500 patients to detect it. It is unclear how a relatively small difference in diuresis may have contributed to the large effect size in the primary outcome of decongestion. Our data, taken with that of the DEA-HF trial, suggest that neither oral nor IV acetazolamide induces a clinically meaningful diuresis compared to high-dose furosemide alone [19]. However, both ADA-HF and DEA-HF recruited fewer than 10% of the number of patients randomised in ADVOR: ultimately, the effect of acetazolamide on diuresis is uncertain. The beneficial effects of acetazolamide, if they exist, may lie in its effect on chloride excretion.
Acetazolamide and chloride
Hypochloraemia is a common side effect of loop diuretics [5, 6]. Post hoc analysis of the ADVOR trial found, as we did, preservation of serum chloride concentration in the acetazolamide arm and decreasing chloride concentrations in the standard-of-care arm. Patients who developed hypochloraemia in the ADVOR trial had a higher rate of re-admission and death at 5 years. However, ACZ treatment did not reduce the event rate, regardless of whether the patient was hypochloraemic or not12. The frequency of hypochloraemia both at baseline and after treatment was higher in ADA-HF than in ADVOR, probably because patients were more severely congested at baseline, and because we used higher doses of furosemide.
Acetazolamide might either prevent or correct hypochloraemia in patients with diuretic-induced hypochloraemia. There are two potential mechanisms by which acetazolamide reduces urinary chloride excretion: (1) by increasing urinary bicarbonate concentration, thereby increasing the negative electrochemical gradient from the urinary space into the renal medulla along which most chloride reabsorption occurs, and (2) by inhibiting the chloride-bicarbonate exchanger on the basolateral membrane of the proximal convoluted tubule reducing the movement of chloride out of the blood [7].
Whether hypochloraemia is a marker of severe disease or a mediator of adverse outcome in patients with HF is unknown. There are possible mechanisms to support the latter: myocyte volume and pH are regulated by chloride-dependent co-transporters, abnormalities of which may cause impaired myocardial contractility, or arrhythmia [3]. Increased chloride delivery to the macula densa suppresses renin secretion, thus, hypochloraemia may increase neurohormonal activation [3]. Hypochloraemia may also contribute to diuretic resistance [3], so maintaining chloride concentrations within the normal range may aid diuresis—this may, in part, explain the positive results of the ADVOR trial.
However, in our study, and in ADVOR, mortality and HF rehospitalisation were numerically higher with acetazolamide [8]. Our population was small, and the study was designed to capture patients with a degree of diuretic resistance; thus, the rates of adverse outcome should be interpreted with caution. Larger trials will be required to determine whether the beneficial effects of acetazolamide on chloride homeostasis in patients with advanced HF translate into outcome benefits beyond decongestion.
A future for acetazolamide?
Prior to the advent of loop diuretics in the 1950 s, acetazolamide was one of the first-line treatments for fluid retention due to HF. Side effects were common: 14–38% of patients at doses > 1000 mg per day and 5–10% of patients at doses ≤ 500 mg per day reported side effects to the treatment [7]. Although there was no statistically significant increase in adverse events with acetazolamide in ADVOR, the rates of worsening renal function, hypokalaemia and hypotension were numerically greater in those who received acetazolamide [8]. The DEA-HF trial reported a greater rate of worsening renal function with acetazolamide [20]. Data on safety and tolerability of acetazolamide in modern studies have been inconsistently reported, and no trial has reported data on non-cardiac or non-renal side-effects [8,9,10,11]. We found that approximately 1 in 3 patients receiving acetazolamide experienced a non-cardiac or non-renal side effect.
Although our sample size was small, our results are consistent with other data. A meta-analysis of 42 trials including 1274 patients treated with oral acetazolamide for various conditions (mean age 44 years [considerably younger than most patients with HF, in whom the risk of side effects from the treatment is greater], mean acetazolamide dose 542 mg per day) found that symptoms such as paraesthesia or fatigue were very common, with numbers-needed-to-harm of 2 and 11 respectively. If a similar diuresis can be obtained with high-dose furosemide alone, it is unclear what role, other than to control serum chloride concentration with unclear clinical benefit, acetazolamide may play in managing patients with congestion due to HF [21].
Limitations
As our pilot study was performed at a single centre, it may be argued that our results are not generalisable. However, our baseline characteristics are similar to those of patients recruited to other, larger trials of patients hospitalised with HF [7, 14, 15, 19].
We recruited patients at any time during hospitalisation as long as they were deemed to require at least 240 mg of IV furosemide per day. This entry criterion was chosen to select patients who had either not responded well to the initial low-dose treatment or were anticipated to have a degree of furosemide resistance on admission due to other clinical factors and thus require high-dose furosemide treatment from the outset. Both sets of patients may be considered to display “diuretic resistance” and, thus, be eligible for adjuvant therapies, such as acetazolamide. However, as a result, patients recruited to ADA-HF had received a median of 180 mg IV furosemide over a median period of 2 days prior to randomisation. By comparison, the ADVOR trial excluded patients who received > 80 mg of IV furosemide equivalents prior to randomisation. This is a key distinction between ADA-HF and ADVOR and may explain the more positive results of the latter.
Our sample size was small and we were unable to rule out a small difference in diuresis: the absolute difference between the arms after 96 h (492 mL) was similar to that seen in the ADVOR trial after 72 h (500 mL) but was not statistically significant. Our trial was of a similar size to DAPA-RESIST, which failed to demonstrate a clinically significant difference in diuresis between metolazone and dapagliflozin.
The absence of a placebo control means that firm conclusions regarding tolerability are difficult to draw. However, the side effects which led to withdrawal from the trial occurred only in the acetazolamide arm, and were due to side effects not known with furosemide (ataxia and paraesthesia). Side effects due to oral acetazolamide are common in other patient cohorts [20].
Approximately 1 in 4 patients in our trial were loop diuretic naïve prior to admission and thus it may be argued that neither high-dose furosemide treatment nor combination diuretic treatment would be appropriate. However, the median duration of hospitalisation prior to randomisation was 2 days, during which time patients had received a cumulative dose of 180 mg of IV furosemide yet were still deemed to require high-dose furosemide treatment due to inadequate initial response to treatment. It remains uncertain for whom high-dose loop diuretic or combination diuretic treatment is suitable.
Finally, like ADVOR, we excluded patients taking SGLT2I at baseline to ensure the only diuretic agents being tested were acetazolamide and furosemide. Although this may limit the generalisability of the results, it provides a clearer comparison between acetazolamide and furosemide versus furosemide alone.


Comments (0)