
Remember me
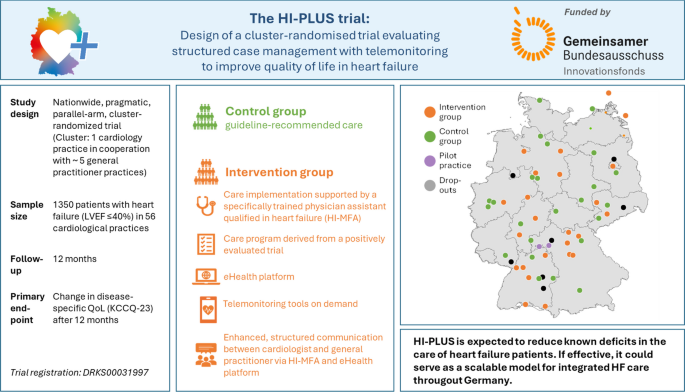

The HI-PLUS trial is a pragmatic, parallel-arm, cluster-randomized study being conducted between June 2023 and June 2026. Cardiology practices (CPs) serve as the units of randomization because the intervention is delivered at the practice level and involves coordination with affiliated general practitioners (GPs). Clusters are generated by a single CP and up to five cooperating GPs and are assigned in a 1:1 ratio to either the intervention or control arm using stratified block randomization generated by PASS 2020 software. Stratification factors include the presence of a HF medical practice assistant (HF-MPA) at baseline. This design permits comparison of the complex intervention with usual care while accommodating the realities of practice-level implementation and minimizing contamination. Further information about the trial organization is listed in Supplementary Table S1.
Setting and recruitmentCPs were recruited through professional associations, specifically the German Association of Registered Cardiologists (BNK). The target was 56 CPs (28 per group) working with approximately 280 GPs. Eligibility required CPs to consent to random allocation, deliver care per assignment, train 1–3 non-physician staff members if randomized to the intervention, and coordinate the network together with approximately 2 to 7 GPs (mean 5). CPs in the control arm that already employed a HF-MPA can participate provided a formal HF care pathway has not yet been implemented. A care pathway is considered implemented if the HF-MPA actively acts as an interface in the following manner between the cardiologist, the GP, the hospital, and the patient: (a) records and assesses HF symptoms, liaises with the supervising cardiologist, and ensures implementation of the recommendations is implemented; and/or (b) monitors the therapy (via telephone or telemonitoring) and provides outpatient coaching as required. The project team surveys CPs quarterly to ascertain whether a HF care pathway has been implemented through completion of an appropriate questionnaire; discovery of an implemented care pathway triggers drop-out from the control arm. It was estimated that approximately 25% of all CPs have already employed a HF-MPA without yet implementing a HF care pathway.
Practice catchment areas should not overlap, and no other HF care program should be offered regularly to participating patients to reduce contamination bias. Patients in the control group receive usual care concordant with national care guidelines [3] and a trial-specific assessment of primary and secondary outcomes. The trial protocol adheres to the CONSORT extension for cluster-randomized trials [17, 18] and was registered at the German Clinical Trials Register (DRKS00031997).
ParticipantsPatients insured under the statutory health insurance and with objectified HF with reduced left ventricular ejection fraction (LVEF ≤ 40%) are identified consecutively in the participating CP or their cooperating GP practices. After initial consultation and trial information by the cardiologist or GP, eligibility confirmation, consent, and enrollment are completed at the CP. In intervention clusters, the HF-MPA assumes responsibility for patient care under delegation. Patients with advanced cognitive impairment or without telephone access were excluded.
Development of the intervention programThe intervention integrates five synergistic elements. First, evidence-based HF care is implemented in each practice, focusing on patient safety, adherence, and optimization of pharmacotherapy. Second, non-physician staff receive a structured, certified curriculum (HeartNetCare™ [10] provided by the German Society of Cardiology (DGK)) through which they gain qualifications in patient education and symptom monitoring. The training curriculum contents are presented in Supplementary Table S2. Completing the curriculum yields a HF-MPA certificate. Third, an eHealth platform (medPower®; ISO-certified medical product) is deployed, allowing HF-MPAs, cardiologists, and GPs to record, share, and act on clinical data in real time. Fourth, portable telemedical devices (e.g., blood pressure monitors and body weight scales) are provided to enable patient-specific telemonitoring and to ensure timely recognition of clinical deterioration by conducting a preliminary assessment of the collected data based on medically defined and individually set thresholds. Finally, structured communication pathways among cardiologists, GPs, and HF-MPAs ensure coordinated care; HF-MPAs perform scheduled telephone follow-ups, document symptoms and vital signs, and consult the supervising cardiologist or GP when warning signs emerge.
Role of the HF-MPAThe HF-MPA is employed in the CP and works under the delegation principle. The HF-MPA provides structured contact at program start, conducts scheduled telephone follow-ups and telemonitoring according to patient needs and disease severity, and promptly escalates warning signs. In consultation with the cardiologist, the HF-MPA collaborates with the GP to identify clinical concerns, to implement therapy adjustments and to optimize guideline-concordant medication, when abnormalities are identified. Figure 1 shows the patient pathway and the distribution of patient groups. The HF-MPA is also responsible for documenting care-relevant information using the patient-specific electronic case file of the eHealth-platform. The eHealth-platform is accessible to the patient’s cardiologist, responsible HF-MPA, and the GP, with the contents of the dashboard displayed according to the assigned role and corresponding permissions. The platform is designed to enhance inter-professional and cross-sectoral care coordination and facilitates timely (tele-)monitoring of patients.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Study flow for control and intervention group
OutcomesThe primary endpoint is the change in HF-specific QoL from baseline to 12 months, measured with the 23-item Kansas City Cardiomyopathy Questionnaire Overall Summary Score (KCCQ-OSS). Its German version has been validated at the Comprehensive Heart Failure Center Würzburg [19]; telephone administration reliability was evaluated prior to the start of the study [20]. The secondary endpoints are presented in Table 1 and include HF-related hospitalization (adjudicated from medical reports) and a health-economic evaluation of first-year intervention costs.
Table 1 Secondary endpoints in the HI-PLUS trialData collectionAt enrollment, targeted phenotyping captures information on socio-demographic determinants and care situation of patients, as well as HF type and severity, previous history of cardiac disease, comorbid conditions, and current medications. CP teams enter endpoint-relevant information into the study database at baseline and 12 months. Additionally, patients are interviewed by telephone by trained staff to collect endpoints at baseline and 12 months. Quality of care provided to patients is evaluated through the administration of the Patient Assessment of Chronic Illness Care measure (PACIC-5A) at enrollment and the final visit. Furthermore, a qualitative study will be conducted among cardiologists, HF-MPAs, general practitioners, and patients to assess the quality of implementation as well as expectations associated with and acceptance of the innovative care pathway. Study data are managed in REDCap© electronic data capture tools hosted at the University of Würzburg [21, 22]. In the intervention group, care-relevant information is also documented with the eHealth platform. Data monitoring is performed by the Clinical Trial Centre of the University Hospital Würzburg.
Sample sizeThe trial is powered to detect a 5-point between-group difference in KCCQ-OSS from baseline to 12 months, a threshold regarded as clinically meaningful and associated with a 10% risk reduction in mortality and HF-related rehospitalization [4, 23,24,25]. Similar or even greater improvements have been observed in previous therapy optimization studies [26]. The sample size calculation is based on a two-sided t-test with degrees of freedom based on the number of clusters, with the significance level set at 5%.
In the INH study, an intraclass correlation coefficient (ICC) of 0.003 was reported for the change in KCCQ-OSS between baseline and 12-month follow-up [10]. Given that the clusters in the INH study comprised cardiology departments within one region, we assume a more conservative ICC of 0.01 for the current trial. For estimating the KCCQ-OSS standard deviation (SD), we refer to the study by Jayaram, which reported an SD of 25.4 points for the change over 6 months [26]. Since the SD remained relatively stable during this period, we assume an SD of 25.4 points after 12 months as well. We also assume a variation in the number of patients per cluster of 0.5. With an ICC of 0.01, an average of 21 HF patients per cluster (n = 1050) is needed to detect a significant 5-point difference with 80% power. Considering an expected dropout rate of 20% for patients and 10% for practices, the final sample size is 56 clusters with 1350 patients. Each cardiologist is expected to collaborate with 2–5 GPs, involving up to 280 GPs in total. The sample size was conducted using the software PASS 2020.
Statistical methodsAnalyses will follow the intention-to-treat principle using SAS 9.3 or R. The significance level is defined at 5%. Descriptive analyses of the primary and secondary endpoints will be carried out. The primary analysis will use a univariable linear mixed-effects model with random effects for clusters (CPs) and fixed effects for group (intervention vs control). A multivariable mixed-effects model will secondarily adjust for potential confounders, e.g., age, sex, NYHA functional class, time since diagnosis, care dependency, and living status. A predefined sensitivity analysis will be performed to account for the timing of the anticipated DMP-HI implementation, whose exact start date had not been determined at the time of trial approval. Specifically, a mixed-effects model will be applied to the primary outcome, including both groups and duration of DMP-HI use as fixed effects, while modelling CP as a random effect. If a CP has not participated in the DMP-HI by the end of data collection, duration will be set to zero. If no CP has adopted the DMP-HI 4 weeks before study end, this analysis will be omitted. In addition, a subgroup analysis will evaluate the primary endpoint based on the presence/absence of a trained HF-MPA prior to trial start. Analyses of secondary outcomes will be conducted using univariable and multivariable mixed-effects models. To assess the potential influence of GPs on study outcomes, an additional sensitivity analysis will be run to account for clustering effects at the GP level. This will involve the use of a mixed-effects model with the intervention as a fixed effect and both cardiologists and GPs as random effects.
Health economic evaluationA cost-effectiveness analysis will be conducted to estimate the mean differences in costs and effects (e.g., QALYs) between the intervention and control groups. The incremental cost-effectiveness ratio (ICER) will be calculated as the difference in mean costs divided by the difference in mean effects, where applicable. Where one strategy is both more effective and less costly, or vice versa, dominance will be reported instead of an ICER. Effects will be assessed as non-monetary and aggregated appropriately according to the study objectives. Utility values for the calculation of QALYs (Quality-Adjusted Life Years) will be derived from data collected using the European Quality of Life Questionnaire (EuroQoL EQ-5D-5L) using the German value set [27]. Relevant cost parameters will be collected individually to maintain the internal validity of the economic evaluation.
To minimize bias due to recall inaccuracies, resource use data will be collected from the most reliable sources available rather than relying solely on patient self-report. Data on hospitalizations will be extracted from hospital discharge letters, which are systematically reviewed by a clinical expert to identify main diagnoses and relevant procedure codes (OPS), allowing individual-level derivation of Diagnosis-Related Groups (DRGs). The number of visits to cardiologists will be obtained directly from participating cardiologists. Telemonitoring equipment, as an additional resource specific to the intervention, will be continuously recorded via the eHealth platform, whereas additional activities of the HF-MPAs will be documented separately by the HF-MPAs themselves. Information on other healthcare utilization, including GP visits, medications, emergency services, rehabilitation stays, nursing care, and therapeutic services (e.g., physiotherapy, occupational therapy, and speech therapy), will be collected from patients using a questionnaire based on the validated FIMA instrument [28]. Data on care level, living situation, and employment status will also be obtained at baseline and at the end of the observation period.
Costs for non-physician staff, such as HF-MPAs, will be calculated based on existing EBM (Einheitlicher Bewertungsmaßstab) codes and an hourly rate. EBM codes refer to the standardized reimbursement system for outpatient services in Germany, assigning monetary values to specific medical procedures. The patient-related costs of the eHealth platform will be calculated. Drug costs will be estimated using average prices. Furthermore, unit costs for various resources will be derived from published cost estimates [29, 30]. To account for the clustered study design and potential confounders, mixed-effects regression models will be applied, with the intervention group as a fixed effect and clusters (CPs) as random effects. Trial data will be assessed for completeness, and appropriate methods will be applied to handle missing values depending on their extent and underlying mechanism. If data are considered missing at random (MAR), multiple imputation techniques may be employed. Uncertainty in the ICER estimates will be assessed using non-parametric bootstrapping (e.g., 1,000 replications), and results will be presented in cost-effectiveness planes and acceptability curves. Sensitivity analyses will explore the robustness of results to assumptions regarding cost structures, the timing of DMP-HI implementation, and data completeness. All health economic analyses will be conducted using StataSE 17.
Process evaluationThe implementation and effectiveness of the intervention across clusters will be assessed using a mixed-methods process evaluation guided by the principles outlined by the UK Medical Research Council [31,32,33]. Key outcomes will focus on patient-level, structural and generalizability factors.
Pilot feasibility studyA pilot feasibility study was conducted to evaluate key aspects of the trial implementation (Supplementary Material 1).
Ethical approvalThe trial was approved by the Ethics Committee of the University Hospital Würzburg in April 2023 (243/22 me). All recruiting centers obtained local ethics committee approval prior to recruitment.
Comments (0)