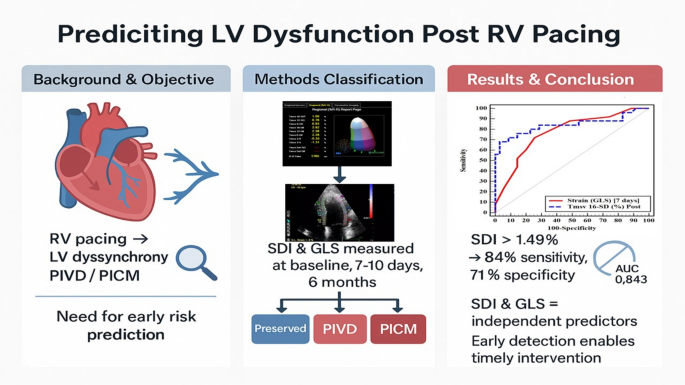
This prospective study, while limited by a modest sample size, provides hypothesis-generating evidence that mechanical dyssynchrony (Tmsv 16-SD) and impaired myocardial deformation (GLS), measurable within one week of right ventricular pacing, may identify patients at higher risk for subsequent LV dysfunction at 6 months. Our work adds to the growing body of evidence on pacing-induced cardiomyopathy (PICM) by highlighting the paramount importance of early mechanical alterations, which appear to precede and predict the decline in conventional volumetric measures like ejection fraction (EF).
The evolving definition of pacing-induced ventricular dysfunction
The definition of PICM has undergone significant evolution since it was first described. Initially, it was recognized as a late complication, often defined by a dramatic decline in LVEF, typically to below 40–45%, in the absence of other clear causes [4, 5]. This classic definition, while specific, risks overlooking a larger cohort of patients who develop significant but subtler deterioration; a condition now often termed pacing-induced ventricular dysfunction (PIVD). Our study intentionally captures this spectrum by classifying dysfunction into two subgroups: PIVD (EF decline without falling below 50%) and the more classic PICM (EF < 50%). This approach is in agreement with contemporary studies that acknowledge PICM as a continuum rather than a binary outcome [10, 16]. By including PIVD, we identify patients at an earlier stage of the disease process, which is crucial for implementing preventive strategies before severe, potentially irreversible damage occurs. Our data show a clear gradient of worsening parameters from Preserved to PIVD to PICM, validating this spectrum-based model and suggesting that the deleterious effects of RV pacing start very early.
Predictors of PICM: moving beyond traditional risk factors
Previous research has identified several baseline clinical and electrical parameters as risk factors for PICM. These include a pre-existing low-normal LVEF [17], a wide native QRS complex [6], a high percentage of ventricular pacing [7], and the presence of coronary artery disease [9, 18]. While our findings are in partial agreement with some of these associations, we observed a non-significant trend toward higher pacing burden in the Dysfunction group. Although our results showed a numerically higher mean pacing burden in the Dysfunction group compared to the Preserved group (97.3% vs. 81.3% at 6 months), this difference did not reach statistical significance (p = 0.078). This observation must be interpreted with considerable caution for several reasons. First, our inclusion criteria required a minimum ventricular pacing percentage of ≥ 20%, but the actual observed pacing burden was substantially higher in both groups (mean > 80%), creating a restricted range that reduces statistical power to detect associations. Second, with only 25 patients in the Dysfunction group, our study is underpowered for this analysis. Third, the definition of high pacing burden in the literature varies considerably, with some studies using thresholds of > 40% [17], others > 80% [19], and still others analyze pacing percentage as a continuous variable [20].
Therefore, a key point of divergence and strength of our study is the demonstration that these traditional factors were not significantly different between our groups at baseline. This lack of discriminatory power for baseline characteristics highlights a critical clinical challenge: relying solely on pre-implantation factors is insufficient to predict which individual patient will develop dysfunction. A patient with a normal EF and a narrow QRS can still develop PICM, as evidenced by our cohort. This is where our work suggests a new prognostic tool. We provide preliminary evidence that the functional response of the myocardium to pacing, quantified by GLS and SDI within the first week, is a more sensitive and earlier indicator of future risk. Our finding that SDI is a potential predictor aligns with the broader utility of this index. For instance, Bhambhani and colleagues [21], who used 3D echocardiography to demonstrate that significant mechanical dyssynchrony, quantified by SDI, is present in over 50% of heart failure patients, even those with a narrow QRS complex. Their observation that the spatial distribution of dyssynchrony is often scattered in such patients underscores that electrical surrogates like QRS duration can be blind to meaningful mechanical disturbances. Our findings suggest a parallel in the pacing population: a significant subset of patients, despite having “normal” traditional parameters, exhibits early post-pacing dyssynchrony that places them on a path toward dysfunction.
Tani and colleagues [22] demonstrated that 3D echocardiography-derived SDI is a useful parameter to assess global LV systolic dyssynchrony, showing a significant inverse correlation with LVEF (r = − 0.686) and a positive correlation with QRS duration (r = 0.407). Furthermore, they established its value in a different context, predicting response to cardiac resynchronization therapy (CRT), where an SDI > 11.9% predicted CRT response with high sensitivity and specificity. Our study extends this concept by showing that SDI can predict the onset of dysfunction caused by pacing itself, not just the response to its correction.
•
Point of agreement and advancement with GLS
Our finding that GLS deteriorates rapidly after pacing and is a strong predictor of dysfunction is consistent with several recent studies [12, 23]. For instance, a study by Leitman et al. [23] found that GLS was significantly worse in patients who developed PICM. Our work strengthens this evidence by showing that this change is detectable extremely early (7–10 days) and provides robust prognostic value (AUC 0.774), independent of other factors. This suggests that GLS captures the immediate, subtle contractile impairment induced by dyssynchronous activation before it translates into EF reduction. Another study by Tatsumi et al. [24], using a three-dimensional speckle tracking system to derive a strain dyssynchrony index, showed that this measure could powerfully predict reverse remodeling after CRT, correlating significantly with the reduction in LV end-systolic volume (r = 0.80, p < 0.001). Their work highlights that indices combining dyssynchrony with residual myocardial contractility (like strain) offer profound clinical insight. While their study focused on predicting CRT response, the underlying principle is directly applicable to our work: the quantification of dyssynchrony and deformation provides a window into the myocardial substrate that is far more nuanced than traditional parameters.
•
Point of major contribution with the systolic dyssynchrony index (Tmsv 16-SD)
The most powerful predictor in our multivariate model was the Tmsv 16-SD, a real-time 3D echocardiographic measure of intraventricular dyssynchrony. While the role of dyssynchrony in PICM pathophysiology is well-established [3], its quantitative assessment has often been limited by 2D techniques. Our use of 3D SDI provides a more comprehensive and reproducible assessment. The strong correlation we found between early post-pacing SDI and subsequent ESV increase and EF reduction underscores that mechanical dyssynchrony is not just a correlate but likely a primary driver of adverse remodeling. The excellent predictive accuracy of an SDI cut-off of > 1.49% (AUC 0.843) suggests it could be a valuable tool for early risk stratification.
•
This pathophysiological concept is strongly supported by the foundational work of Tops et al. [3], who established the direct link between RV pacing, immediate mechanical dyssynchrony, and subsequent LV dysfunction. Our findings on the acute induction of mechanical dyssynchrony are consistent with the foundational work of Fang et al. [25], who first used real-time 3D echocardiography to quantify the high prevalence of LV systolic dyssynchrony immediately after RV apical pacing in patients with normal baseline EF.
•
However, our study critically extends these observations. While Fang et al. descriptively characterized the acute phenomenon, we demonstrate that the magnitude of this early dyssynchrony is not merely an epiphenomenon but a powerful prognostic biomarker. We transition the application of RT3DE from describing the pathophysiology to enabling early, personalized risk prediction.
Potential implications and future directions
The early timing of our predictive measurements (7–10 days post-pacing) is a key clinical advantage. This “window of opportunity” allows for proactive management in high-risk patients identified by GLS and SDI before significant irreversible remodeling sets in. One might hypothesize that interventions could include optimizing medical therapy (e.g., intensifying renin–angiotensin–aldosterone system blockade), reassessing the need for high pacing percentages, or considering early upgrade to biventricular or conductive-system pacing.
Furthermore, our correlation analysis provides insight into pathophysiology. The strong inverse relationship between SDI and EF, and its positive correlation with ESV, paints a clear picture: greater immediate dyssynchrony leads to inefficient contraction, increased energy expenditure, and ultimately, remodeling and dilatation of the LV. The absence of a significant correlation between SDI and lead location or pacing percentage within the dysfunction group, while requiring very cautious interpretation, raises an intriguing hypothesis: the mechanical response to RV pacing may be substantially heterogeneous and patient-specific, not solely determined by the site or cumulative burden of pacing. This observation aligns with the well-recognized clinical phenomenon that some patients with high-burden apical pacing maintain normal LV function for decades, while others develop PICM despite seemingly ‘favorable’ lead positions and only moderate pacing burden.
Several important methodological caveats must be emphasized when interpreting the lack of association with lead position. First, lead location was determined by standard fluoroscopic guidance in two orthogonal views, which is now recognized as an imprecise method for confirming true septal positioning. Burri and colleagues [26] demonstrated that when only standard fluoroscopic views (PA and LAO) were used, only 45% of leads intended to be septal were actually positioned on the septum by echocardiographic validation; the majority were on the anterior free wall. This misclassification bias would systematically dilute any true differences between apical and septal pacing, biasing our analysis toward the null hypothesis. Second, the largest randomized trial to address this question, the UKPACE trial [27], similarly found no difference in mortality, heart failure hospitalization, or LV function between apical and non-apical pacing over a mean follow-up of 4.6 years. Our findings are therefore consistent with the highest-quality evidence available, which suggests that simply targeting the septum under fluoroscopic guidance does not reliably prevent pacing-induced dysfunction. Third, with only 25 patients in the dysfunction group and only 7 non-apical lead placements, our study was profoundly underpowered for this subgroup analysis; the absence of statistical significance may well represent a Type II error rather than a true biological null effect.
3D echocardiography for dyssynchrony assessment: required or complementary?
An important practical question is whether three-dimensional echocardiography is strictly necessary for dyssynchrony assessment or whether two-dimensional methods might suffice. Vaidya and colleagues [28] directly compared 2D-strain-derived and 3D-echocardiographic parameters, reporting excellent correlation for LVEF and volumes but, critically, no significant correlation between 2D-strain-derived and 3D-derived systolic dyssynchrony indices (r = 0.171). This finding has important implications: while 2D echocardiography may adequately assess LVEF and volumes in paced patients, the quantification of mechanical dyssynchrony appears to require 3D acquisition. The 2D methods assess dyssynchrony in single imaging planes, whereas 3DE captures the entire LV volume and provides a global measure of temporal contraction disparity across all segments simultaneously. Therefore, while we acknowledge that 3DE is not universally available and requires specific expertise, our data suggest that if the goal is to quantify global LV mechanical dyssynchrony, 3D echocardiography may be uniquely suited for this purpose. Two-dimensional echocardiography remains entirely appropriate for routine assessment of LV volumes and ejection fraction in paced patients. However, for dyssynchrony quantification, 2D methods appear to capture a different aspect of myocardial mechanics and cannot be considered interchangeable with 3D-derived SDI. Whether 2D surrogates can be refined to approximate 3D SDI remains an important area for future investigation.
Relevance of conduction system pacing
Our study must be interpreted in the context of rapidly evolving pacing technologies. Left bundle branch area pacing (LBBAP) has emerged as a promising alternative to conventional RV pacing, achieving physiological ventricular activation via the native conduction system with narrow-paced QRS duration and preserved ventricular synchrony. Recent comparative studies have demonstrated a significantly lower PICM incidence with LBBAP (4.3%) compared to RV septal pacing (24%) in patients with high pacing burden [29]. Furthermore, among patients who have already developed PICM from chronic RV pacing, upgrading to LBBAP may be superior to biventricular pacing for LVEF recovery (9.6% vs. 4.9% absolute improvement at 6 months, p = 0.008) [30].
These emerging data raise the question: if LBBAP can prevent PICM, is there still a role for early risk stratification with SDI and GLS? We propose that these approaches are complementary rather than competitive. First, LBBAP is not universally feasible or successful; implantation failure rates and the need for lead revision are not negligible, and many patients continue to receive conventional RV pacing systems. Second, even with LBBAP, some patients develop residual dyssynchrony and may benefit from early identification. Third, for the large prevalent population of patients with existing RV pacing systems, risk stratification remains highly relevant to guide decisions about upgrade procedures. Thus, while we enthusiastically support the adoption of physiological pacing when feasible, we believe that early post-pacing mechanical assessment retains clinical relevance in the current era.
Study limitations
Our study has several limitations. Most importantly, the modest sample size (n = 60) significantly limits the robustness of our findings and precludes definitive conclusions. While we observed strong associations between early SDI/GLS and subsequent dysfunction, the relatively small number of events (25 dysfunction cases, including only 9 PICM cases) increases the risk of both false-positive and false-negative findings. The proposed cut-off values (> 1.49% for SDI, > − 17% for GLS) should be considered preliminary and require independent validation in larger, preferably multicenter, cohorts before any clinical application can be considered. Our study is best viewed as hypothesis-generating, providing rationale for larger prospective investigations rather than evidence for immediate clinical implementation. Second, the follow-up period was 6 months; longer-term follow-up would be valuable to assess the durability of these predictions and the natural history of PIVD. Third, three-dimensional echocardiography is highly dependent on adequate acoustic windows and image quality. Suboptimal visualization of the endocardial border, particularly in the lateral and anterior walls, can compromise the accuracy of semi-automated border detection and the derived SDI values. Although we excluded patients with poor echocardiographic windows at enrollment, this introduces selection bias and limits the generalizability of our findings to the broader pacemaker population, which includes many patients with suboptimal acoustic windows. Furthermore, the expertise required for 3D acquisition and offline analysis may not be available in all echocardiography laboratories, potentially limiting the widespread applicability of this technique. Finally, our inclusion criterion of ≥ 20% ventricular pacing, combined with the very high observed pacing burden in the majority of patients (mean > 80%), resulted in a restricted range that limited our ability to detect associations between pacing percentage and outcomes.
Conclusion
In conclusion, this hypothesis-generating study suggests that the development of pacing-induced ventricular dysfunction may be detectable very early after pacemaker implantation through assessment of mechanical dyssynchrony (3D SDI) and myocardial deformation (GLS). These preliminary findings, if confirmed in larger prospective cohorts, could inform the design of interventional trials aimed at preventing progression to overt cardiomyopathy. For the present, our results should be considered exploratory and require independent validation.


Comments (0)