This literature review highlights the potential severity of PH, which can present with a broad spectrum of clinical manifestations, ranging from mild symptoms to life-threatening anaphylaxis. It also underscores the heterogeneity in allergy work-up and the wide range of therapeutic strategies described in the literature, reflecting the overall complexity of this condition.
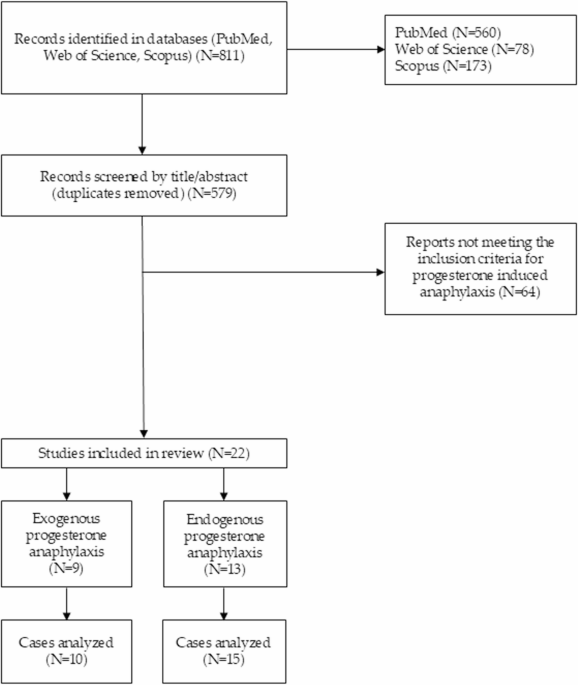
The earliest report of progesterone-induced anaphylaxis identified in our review dates back to 1974 [36], indicating that the condition has been recognized for several decades. A literature review published in 2003 specifically addressing progester-one-induced anaphylaxis reported only two cases attributed to exogenous progesterone and six to endogenous progesterone, highlighting the rarity of documented cases at the time and the exceptional nature of reactions to exogenous forms, likely due to their more limited use [37]. Since then, the number of published reports has increased. The present review identified more recent and better-characterized cases, which may reflect a rising incidence of the condition.
Patients Profile and Clinical Characteristics
Although PH primarily affects women, and all patients in our review were female, one case has been reported in literature in a male patient presenting skin-limited symptoms while undergoing exogenous progesterone treatment (prescribed to stimulate appetite and weight gain in patients with cancer- or AIDS-related anorexia, regardless of gender) [44]. The median age of the patients in the reviewed cases was relatively young (34 years for exogenous and 30.5 years for endogenous, respectively), which aligns with previous findings suggesting that PH predominantly affects women in their peak reproductive years [15, 28, 45]. Regarding the pregnancy status of the patients at diagnosis, one patient, who experienced anaphylactic symptoms prior to conception, also presented recurrent anaphylaxis episodes specifically during the second and third trimesters of her pregnancy [46]. Furthermore, one parturient patient with a 14-year history of autoimmune progesterone dermatitis developed severe anaphylaxis during an emergency caesarean section. However, the reaction occurred 40 min after delivery, resulting in no harm to the newborn, who presented with Apgar scores of 8 and 10 [47]. Parity among patients was variable. While sensitization is often hypothesized to occur during periods of high endogenous progesterone levels, such as pregnancy [48], we also identified a case of anaphylaxis to endogenous progesterone in a nulliparous patient [49], suggesting that pregnancy is not a requirement for sensitization. Interestingly, in the exogenous progesterone group, one patient had a prior history suggestive of hypersensitivity to endogenous progesterone and despite high progesterone levels during pregnancy, this patient experienced complete symptom remission during that period [38]. This paradoxical improvement has also been reported by other authors in patients with non-anaphylactic PH [50,51,52,53,54,55]. One possible explanation is that pregnancy may act as a form of natural desensitization to progesterone, due to the gradual and sustained increase in endogenous hormone levels [48, 56]. Alternatively, this phenomenon could be related to a reduced maternal immune reactivity to progesterone during pregnancy [48, 56,57,58,59]. Hormonal transitions surrounding childbirth and breastfeeding may also influence symptom onset. In one case, symptoms began a few days postpartum [60], whereas in another, complete remission was observed during the breastfeeding period [49].
Previous exposure to exogenous progesterone was reported in 33.3% of patients with endogenous progesterone-induced anaphylaxis. This finding is consistent with variable results across other case series describing PH, highlighting that sensitization to endogenous progesterone can develop independently of prior exogenous exposure [45, 61, 70,71,72].
Several patients experienced non-anaphylactic symptoms suggestive of PH prior to the index anaphylactic reaction. In our review, such symptoms were reported in 7 out of 15 patients (46.6%) with endogenous progesterone-induced anaphylaxis, and in 2 out of 10 patients (20%) with exogenous progesterone-induced anaphylaxis, supporting the possibility of prior sensitization before the anaphylactic reaction (Tables 1 and 2). However, a review by Sandru et al. [73] which investigated PH reactions related to exogenous hormone administration during assisted reproductive techniques, found that most patients had no prior history of hypersensitivity, suggesting that sensitization to exogenous progesterone may occur even in the absence of previously recognized reactions to endogenous hormone. Following an anaphylactic reaction to a combined oral contraceptive, one patient from the exogenous group went on to develop persistent maculopapular dermatitis attributed to endogenous PH, persisting for more than 21 years [14]. This case provides evidence that exposure to exogenous progesterone may prime the individual’s response to endogenous progesterone despite molecular differences between the two. It also aligns with the mixed clinical phenotype proposed by Foer et al. [24].
The clinical manifestations described in our review highlight the potential severity of PH. One patient experienced grade 5 anaphylaxis, and 12 additional reactions were classified as grade 4, emphasizing the serious nature of this condition. Notably, in the case of the grade 5 anaphylaxis, the true trigger was initially misattributed to anesthesia. As a result, the patient was re-exposed to exogenous progesterone, which led to another severe reaction (grade 4) [39]. This case underscores the urgent need for increased awareness of this hormone (natural or synthetic) as a potential trigger of hypersensitivity reactions among healthcare professionals across specialties.
Diagnosis
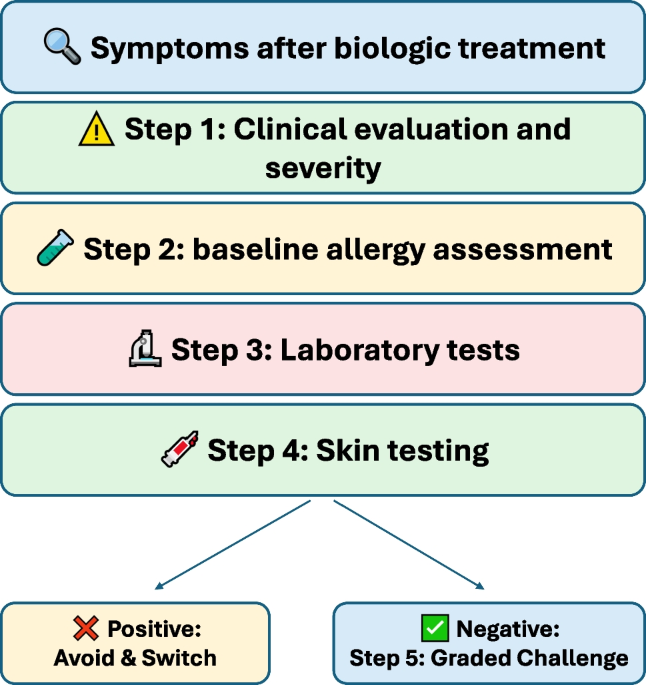
The diagnosis of PH is primarily based on a highly suggestive clinical history. In the articles included in this review, skin testing and provocation tests were used in some patients to support the diagnosis, while in others, a therapeutic response served as the main diagnostic tool. This therapeutic response refers to the administration of progesterone-suppressive therapy, followed by remission of symptoms due to the cessation of exposure to the triggering agent—progesterone. As noted by some authors, a therapeutic response may be sufficient to establish the diagnosis, and in cases with a strong clinical history, additional diagnostic procedures may not be necessary [53, 74, 75].
In the articles reviewed, skin testing yielded positive results in most patients tested. However, the reviewed cases illustrate marked heterogeneity in the allergy work-up, with skin testing performed only in a subset of patients and using widely variable concentrations, ranging from 0.05 mg/ml to 50 mg/ml. The guideline proposed by Broyles et al. [76], a key reference for standardizing cutaneous testing, recommended a maximum concentration of 50 mg/ml for prick testing and 5 mg/ml for intradermal testing. Higher concentrations (such as the 50 mg/ml solution for ID reported in some studies) produced positive reactions also in a control group of 10 healthy women, raising concerns about false positives [77]. The risk of false positive results can additionally be reduced by performing control tests with the diluent, particularly because progesterone is not water-soluble and is often formulated in oil- or ethanol-based solutions [78]. Of note, in one patient included in this review, previously positive skin test results became negative five months after discontinuation of omalizumab therapy [79].
The role of in vitro tests in the diagnosis of PH remains insufficiently defined. Although progesterone-specific IgE antibodies have been identified in some patients, and other tests such as leukocyte histamine release and interferon-gamma release assays have been used to support the diagnosis [15, 61, 80, 81], their clinical utility and accessibility still remains limited. In vitro investigations were reported in only 3 of the 25 cases included in this review, suggesting a modest role for such assays when a suggestive clinical history and symptom pattern are present [8, 14, 63, 74].
Provocation testing can be particularly useful in cases with an inconclusive clinical history. While direct provocation with exogenous progesterone appears to be the most straightforward approach, some practitioners have also employed LHRH administration as an indirect challenge method in patients with suspected endogenous progesterone-induced symptoms [74, 76]. In the studies included in our review, oral or intramuscular progesterone challenge confirmed the diagnosis in 2 out of 2 cases [38, 62] while LHRH challenge yielded positive results in 3 out of 4 patients [46, 49]. One patient with suspected endogenous PH had a negative LHRH challenge and did not respond to long-acting LHRH agonist therapy. Despite this, the patient’s skin test to medroxyprogesterone was positive, and the clinical history was highly suggestive of the diagnosis [82]. A possible explanation for the negative challenge result is that the progesterone levels induced by LHRH stimulation may not have reached the individual symptomatic threshold. This mechanism has also been proposed as an explanation in cases of false-negative results during exogenous progesterone challenge [53, 74]. Specific progesterone challenge protocols have been proposed by Chiarella et al. [56], aiming to standardize diagnostic procedures.
A significant limitation across the reviewed literature is the inconsistent reporting of comorbid mast cell disorders. Heffler et al. [69] were the only authors to explicitly state that masquerading conditions, specifically systemic mastocytosis, were considered and ruled out in their patient. The remaining studies did not document serum tryptase levels or specific screening for mast cell activation syndrome. This lack of screening is particularly concerning because the exclusion of mast cell disorders is clinically paramount to prevent misdiagnosis and inappropriate management. Distinguishing between a specific IgE-mediated allergy to progesterone and non-specific mast cell degranulation triggered by hormonal fluctuations ensures that patients receive targeted therapies. Crucially, an accurate differential diagnosis avoids unnecessary and irreversible surgical interventions, such as bilateral oophorectomy [60].
Finally, the role of excipients in exogenous progesterone formulations must also be considered, as they may significantly impact diagnostic accuracy. Sensitization to excipients was suspected in two patients included in the reviewed articles. One patient had a prior history of anaphylaxis to Alfathesin (alfaxalone/alfadolone acetate), a discontinued anesthetic agent. The authors hypothesized that the reaction may have been due to hypersensitivity to a solubilizing agent common to both Alfathesin and the medroxyprogesterone formulation [36]. In another case, the patient declined skin testing to progesterone itself but agreed to testing for the excipients present in the suspected preparation, including polyethylene glycol 3350, polysorbate 80, methylparaben, and propylparaben. A positive intradermal reaction to polyethylene glycol 3350 (at a 1:10 dilution) was observed. Interestingly, the same substance was later tolerated when administered orally, suggesting that the route of exposure may influence the clinical expression of hypersensitivity [41].
Management
The acute management of anaphylaxis should follow established therapeutic guidelines [33]. Yet, in our review, epinephrine was administered in only 4 out of 15 cases (26.6%) involving endogenous progesterone-induced reactions, and in 4 out of 13 episodes (30.7%) attributed to exogenous progesterone. This low rate of epinephrine use may reflect limited awareness among healthcare professionals regarding progesterone as a potential trigger of anaphylaxis. In consequence, the clinical suspicion for anaphylaxis may be delayed or misdirected, especially when the hormonal exposure is not initially perceived as allergenic. An illustrative case is the one reported by Selo-Ojeme et al. [30], in which the initial reaction was misattributed to anesthesia. As a result, progesterone was subsequently re-administered, leading to a second anaphylactic episode [39].
Long-term management should be tailored to each patient’s therapeutic goals. For some patients, symptom control may be the primary objective, while others may desire to pursue pregnancy, with or without assisted reproductive techniques such as IVF.
Across the cases included in this review, symptom control was tempted unsuccessfully using antihistamines, corticosteroids and leukotriene receptor antagonists. Suppression of endogenous progesterone secretion was approached through various strategies, including long-acting GnRH agonists (LHRH analogues), conjugated estrogens, and oophorectomy. Additionally, omalizumab was employed in selected cases, particularly when conventional treatments failed or when hormonal suppression could no longer be prolonged [8, 60, 79]. Although oophorectomy is viewed as a definitive approach, complete symptom resolution was achieved in four out of six patients [46, 62, 63, 82], while two presented only partial improvement [49, 60]. Notably, in one patient, symptom control was achieved through the administration of synthetic progesterone [67], whereas in others, exposure to exogenous progesterone as part of combined oral contraceptives triggered hypersensitivity reactions [60, 83].
Regarding strategies for symptom control induced by exogenous progesterone, changing the route of administration (oral, vaginal, or injectable) and, consequently, the excipients, was unsuccessful when the active product remained the same. Specifically, Gupta et al. [43] reported a patient who developed hypersensitivity reactions to natural micronized progesterone regardless of its formulation, reacting sequentially to aqueous intramuscular injections, vaginal gel and oral capsules. Furthermore, the rotation between different classes of synthetic progestins and natural progesterone has also proven ineffective. Poole and Rosenwasser [38] described a patient who exhibited pan-sensitivity to 19-nortestosterone derivatives (Norethindrone), 17-hydroxyprogesterone derivatives (Medroxyprogesterone Acetate), spironolactone analogues (Drospirenone) and natural micronized progesterone. This suggests that in cases of total cross-reactivity, switching the chemical class of the progestogen may not prevent anaphylaxis.
However, in case of exogenous induced symptoms, if the hormonal supplementation is mandatory, a desensitization protocol is the only option. Among the cases included in our review, this approach was successfully applied in one patient, who subsequently carried a pregnancy to term and gave birth to twins [40]. The protocols vary in terms of number of steps, duration and administration route (oral, intravaginal), but also in goal, the desensitization being mandatory not only for IVF procedures but also for other conditions that need hormonal supplementation such as uterine bleeding [38, 72]. Additionally, desensitization protocols using intramuscular progesterone have been proposed, with both rapid and slow escalation approaches reported [24, 75, 84, 85].
Desensitization protocols have also been applied in cases of endogenous progesterone-induced anaphylaxis, particularly when other therapeutic strategies have failed. In the present review, two patients were identified as having unsuccessful desensitization attempts; however, details regarding the protocols used were not provided [8, 61]. For one of these patients, a successful outcome was eventually achieved through the addition of omalizumab to the desensitization protocol involving a combined oral contraceptive [8].
A noteworthy observation was made in one case, where anaphylactic symptoms resolved spontaneously following skin testing, but the manifestations shifted to a fixed drug eruption at the injection site. This suggests a possible modulation of the immune response after allergy evaluation [66].
Other treatment options for PH, though not yet reported in patients with anaphylaxis, have shown promising results in milder forms of the condition. These include danazol [70,


Comments (0)