The study was conducted at multiple centers in the United States, Canada, Poland, United Kingdom, South Korea and Taiwan under local laws and regulations and in accordance with ethical principles set forth in the Declaration of Helsinki, the Council for International Organizations of Medical Sciences guidelines and International Council for Harmonisation Good Clinical Practice guidelines. The trial protocol, all amendments and other relevant documents were approved by the institutional review board or independent ethics committee at each study site. All participants provided written informed consent before enrollment. CONSORT guidelines41 were followed in the reporting of this study and the CONSORT checklist is available in the Supplementary Information. Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Participants
Eligible participants for BEGONIA were females aged ≥18 years with untreated, unresectable, locally advanced or metastatic stage IV TNBC. Participants enrolled into arm 6 were specifically required to have documented HER2-low tumor expression (IHC 1+/ISH−, IHC 2+/ISH− or IHC 1+/ISH untested) as determined by local testing. Other eligibility criteria included at least one unirradiated Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 lesion, Eastern Cooperative Oncology Group performance status of 0 or 1 and adequate organ and marrow function. TNBC was defined as ER-negative, PR-negative and HER2-negative according to the American Society of Clinical Oncology and College of American Pathologists testing guidelines42,43.
Prior treatment for stage I–III TNBC was permitted if, at the time of screening, ≥6 months had elapsed from the completion of treatment to the first documented distant recurrence. Taxane-based therapy within the previous 12 months from the date of screening and any prior exposure to immune-mediated therapy were prohibited. Participants were required to discontinue ongoing hormonal therapy for previous ER+ or PR+ breast cancer, with a 28-day washout period before study randomization. Exclusion criteria included untreated metastases of the central nervous system, active or prior autoimmune or inflammatory disorders, history of another primary malignancy, leptomeningeal carcinomatosis or active primary immunodeficiency, prior allogeneic organ transplant, uncontrolled intercurrent illness, active tuberculosis, hepatitis B virus, hepatitis C virus or HIV infections and known allergy to study therapies or their components.
Specifically for arm 6, participants were excluded if they were previously diagnosed with HER2+ breast cancer or had received HER2-targeted therapy, had a history of noninfectious pulmonary disorders, had any lung-specific intercurrent clinically important illnesses or received prior treatment with an antibody–drug conjugate that included an exatecan derivative.
Study design
BEGONIA (NCT03742102) is a multicenter, multiarm, open-label, phase 1b/2 platform trial initiated to concurrently evaluate first-line novel treatment combinations for locally advanced unresectable or metastatic TNBC using a Simon’s two-stage design (Extended Data Fig. 2). The primary objective of part 1 was to assess the safety and tolerability. The primary objective of part 2 was to assess the efficacy of durvalumab combinations. Tumor biomarker analysis was an exploratory objective. The BEGONIA study used a Randomization and Trial Supply Management System (Interactive Response Technology) to centrally assign eligible participants to one of the open treatment arms. Participants were allocated into arm 6 on the basis of locally assessed HER2 tumor expression and, therefore, were not randomized. Participants with tumors classed as HER2-negative according to local HER2 expression were eligible for assignment to any open treatment arm other than arm 6.
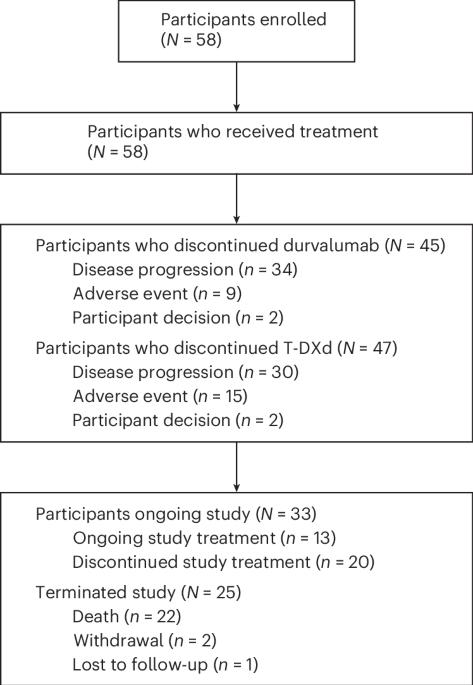
For the arm 6 durvalumab plus T-DXd treatment combination cohort, the first six participants were monitored for dose-limiting toxicities during a run-in period, with additional participants enrolled if treatment was tolerated (around 30 evaluable participants in total for part 1). To determine whether expansion to part 2 of the Simon two-stage design was warranted for a given novel treatment combination, an assessment of confirmed ORR of participants from part 1 was performed after enrollment was complete. All participants had the opportunity to complete ≥2 on-treatment response evaluations or discontinue treatment. The arm was permitted to proceed to part 2 expansion (with approximately 27 additional evaluable participants enrolled) if confirmed ORR was at least 57% in part 1.
No compensation was offered to participants for trial participation. The study protocol is included in the Supplementary Information.
Treatment
Participants received intravenous durvalumab (1,120 mg) every 3 weeks (Q3W) and intravenous T-DXd 5.4 mg kg−1 Q3W. Dose reductions were not permitted for durvalumab. For T-DXd, dose modifications including dose reductions were permitted on the basis of dose-limiting toxicity or toxicity management guidelines as applicable. The T-DXd dose could be reduced to a maximum of two dose levels, with one at 4.4 mg kg−1 Q3W and the other at 3.2 mg kg−1 Q3W. All participants were treated until disease progression or other discontinuation criteria were met; however, treatment beyond progression was permitted at the discretion of the investigator and participant.
Assessments
Safety was assessed through physical examinations, vital signs, clinical laboratory tests, electrocardiograms and echocardiogram or multiple-gated acquisition. AEs were reported per the National Cancer Institute Common Terminology Criteria for AEs grading scale version 4.03. Immune-mediated AEs were defined as AEs of special interest consistent with an immune-mediated mechanism of action with no clear alternate etiology and that required the use of systemic corticosteroids, other immunosuppressants or endocrine therapy to manage the AE. All potential cases of ILD or pneumonitis in BEGONIA arm 6 were evaluated by an independent adjudication committee triggered by prespecified ILD or pneumonitis Medical Dictionary for Regulatory Activities Terminology (MedDRA) preferred terms, regardless of event grade. ILD and pneumonitis are AEs of special interest for T-DXd and included the preferred terms of acute respiratory failure, bronchiolitis, ILD, lung opacity, organizing pneumonia and pneumonitis. Pneumonitis as an AE of special interest for durvalumab included the preferred terms ILD and pneumonitis.
Tumors were assessed by the investigator using computed tomography or magnetic resonance imaging at baseline, then every 6 weeks for the durvalumab plus T-DXd arm for a total of 48 weeks and then every 12 weeks thereafter per RECIST version 1.1.
Biomarker and translational analysis
The analysis of blood and tumor biomarkers was an exploratory outcome. HER2 expression was assessed locally by IHC and ISH for study enrollment. HER2-low tumor expression was defined as IHC 1+/ISH−, IHC 2+/ISH− or IHC 1+/ISH untested. ISH was determined by fluorescence or dual ISH methods. HER2 expression was assessed centrally and retrospectively on archival tumor tissue samples by IHC using the VENTANA/PATHWAY anti-HER2/neu (4B5) assay (rabbit monoclonal primary antibody; clone 4B5, 0599957000, Roche Diagnostics). This assay is indicated for identifying persons with breast cancer who are eligible for treatment with HER2-targeted therapies. The antibody comes prediluted and was used according to manufacturer’s instructions. Tumor expression was defined as IHC 3+, 2+, 1+, ultralow (IHC 0 with membrane staining) or 0 absent membrane staining.
PD-L1 expression was assessed centrally and retrospectively on archival tumor tissue samples by IHC using the VENTANA PD-L1 (SP263) assay (rabbit monoclonal primary antibody; clone SP263, 07419821001, Roche Diagnostics). The antibody was used according to manufacturer’s instructions. Expression was defined as the percentage of the tumor area populated by tumor cells with membranous PD-L1 staining or immune cells with membranous, cytoplasmic or punctate PD-L1 staining at any intensity (TAP score). A sample was considered PD-L1-positive if the TAP score was ≥10% and PD-L1-negative if the TAP score was <10%.
Statistical analysis
The study was sized to allow the use of a Simon two-stage design for each treatment arm according to the targeted ORR improvement from 55% to 75% with 94% power and 5% α. The treatment arm required 57 response-evaluable participants (30 in part 1 and 27 in part 2). If at least 17 of 30 participants achieved response in part 1, then the treatment arm could continue to part 2; otherwise, further recruitment into the treatment arm would be stopped. If there were at least 38 of 57 evaluable participants achieving response in a treatment arm, then the data for that cohort would be considered as having an adequate efficacy signal.
Descriptive statistics were used for baseline participant and disease characteristics. The safety analyses were performed in participants who received any amount of study treatment (safety analyses set). For the durvalumab and T-DXd arm, safety data were pooled from part 1 and part 2. Efficacy data were pooled from part 1 and part 2 of the study.
ORR was a key secondary endpoint for part 1 and the primary endpoint for part 2 and was defined as the percentage of participants with at least one confirmed complete or partial response of all treated participants with measurable disease at baseline who had the opportunity to complete at least two on-treatment disease assessments (response-evaluable analysis set). DoR, PFS, PFS at 6 months and OS were secondary endpoints in this study and were assessed for all participants who were assigned to treatment and received any amount of study treatment (intent-to-treat population). DoR was measured from the date of first documented confirmed response to the date of progression or death. PFS was measured from the date of first dose of study drug until the date of progression or death. OS was measured from the date of first dose of study drug until the date of death. All time-to-event endpoints were calculated using the Kaplan–Meier method. Data collection and analysis were not performed blind to the conditions of the experiments. Statistical analyses were performed with SAS software (version 9.4).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.



Comments (0)