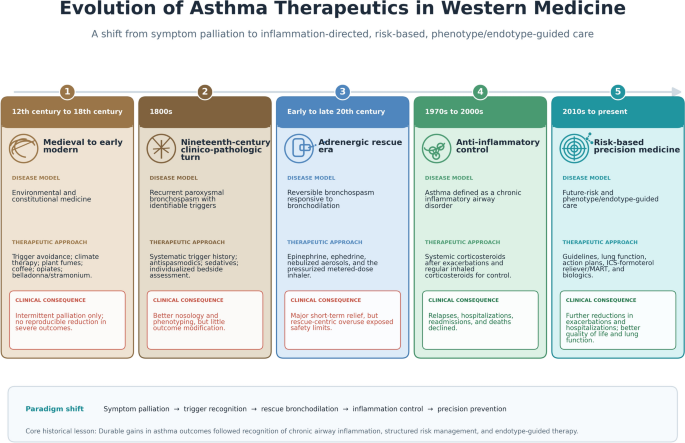
Asthma therapeutics in Western countries have progressed through five main successive discoveries: from a medieval focus on environmental and constitutional medicine, nineteenth-century clinico-pathologic management of recurrent bronchospasm, twentieth-century adrenergic bronchodilator rescue, corticosteroid-mediated anti-inflammatory control, to the current risk-based precision medicine (Table 1).
Table 1 Major therapeutic eras in the history of asthma careFor centuries, clinicians relied on trigger avoidance, climate therapy, inhaled plant fumes, coffee, opiates, and belladonna or stramonium preparations; these measures sometimes averted and treated asthma attacks but lacked reproducible evidence for consistently reducing acute attacks, let alone hospitalizations or fatalities due to asthma [1,2,3,4].
The introduction of epinephrine, ephedrine, nebulized aerosols, and then the pressurized metered-dose inhaler dramatically improved short-term symptom relief, yet it also entrenched a rescue-centric model that proved unsafe when patients overused high-dose nonselective beta-agonist aerosols [4,5,6]. The decisive improvement in outcomes came when asthma was reconceptualized as a chronic inflammatory airway disorder. Short courses of systemic corticosteroids after acute exacerbations can reduce relapses and subsequent hospitalizations, while regular ICS reduce the risk of asthma hospitalizations, re-admissions, and deaths from asthma [7,8,9].
Guideline-based chronic disease management further improved outcomes by integrating objective lung function, written action plans, and structured self-management [10,11,12]. More recently, the replacement of short-acting beta2-agonist monotherapy by the combination of ICS–beta2 agonists as anti-inflammatory reliever therapies have reduced emergency department visits and hospitalizations from asthma [13, 14]. In severe asthma, biologics added to usual care with ICS and beta2-agonists now provide endotype-directed treatment with further substantial reductions in exacerbations and hospitalizations [15]. The core historical lesson is that significant improvements of asthma therapies have led to better symptom management, increased pulmonary function, better quality of life, reductions of exacerbations, hospitalizations, and mortality.
The development of therapies for asthma produced a major shift away from symptom relief alone toward inflammation-directed, risk-based, and phenotype/endotype-guided care. The history of therapies for asthma in western countries is not only a chronology of drug discovery but it is also the record of repeated changes in the disease model that clinicians used at the bedside. Clinicians in pre-modern medicine interpreted asthma through constitutional and environmental frameworks, and treatment focused on regulating the patient’s breathing air, food intake, habits, and immediate symptoms [1, 3]. By the nineteenth century, physicians such as Henry Hyde Salter (himself an asthmatic) had given asthma a more precise nosology as a recurrent paroxysmal disorder of the airways, which in turn encouraged more systematic clinical history-taking around triggers and local influences [2]. The twentieth century then produced an enormous improvement in asthma management through the use of spirometry as well as symptomatic control through adrenergic bronchodilators and portable aerosol delivery systems, but also exposed patients to the dangers of equating bronchodilator responsiveness with long-term safety [4,5,6]. The modern era began when pathobiology, therapeutics, and guidelines converged around a new proposition: asthma is a chronic inflammatory airway disease with future exacerbation risk, and treatment must fundamentally suppress inflammation, not merely reverse bronchospasm [7,8,9,10,11,12,13,14].




Comments (0)