
Remember me



A retrospective observational cohort study was conducted using linked medical and pharmacy claims from IQVIA Anonymized Patient Level Database (APLD) and TROF specialty pharmacy database from 01/01/2021 to 09/30/2024 (study period). The APLD database contains de-identified, anonymized, pre-adjudicated healthcare claims capturing longitudinal information on patient demographics, diagnoses, procedures, and outpatient pharmacy dispensing for over 130 million beneficiaries in the USA. As this study involves deidentified, anonymized, patient level secondary data from other claims data sources without containing any identifiable protected health information (PHI) in accordance with HIPAA Security Act of 1996, patient consent was not required, and the need for ethics committee approval was not applicable.
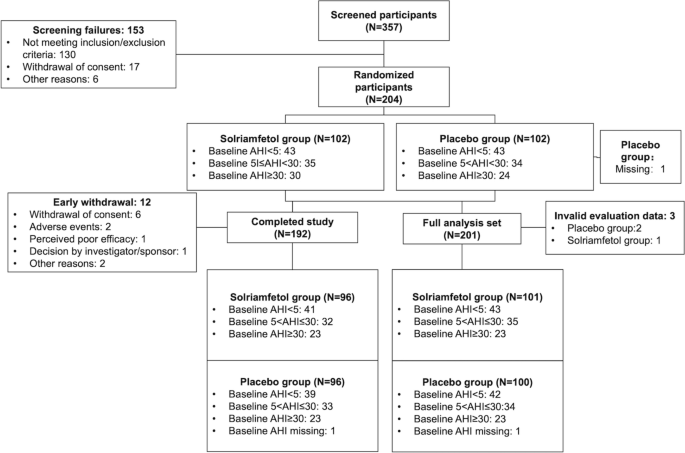
Study Population and Cohort SelectionIndividuals with at least one or more medical claims containing the ICD-10-CM code F84.2 for RTT were initially identified. From the eligible population, males were identified for this analysis and categorized into two groups based on TROF use (treated vs untreated) between 04/01/2023 and 03/31/2024 (identification period; Fig. 1). The treated male group was defined as those individuals who have at least one pharmacy claim for TROF during this identification period. The index date was defined as the date of their first TROF prescription (RX) fill for this group. The untreated male group was defined as those who did not initiate TROF during the identification period. To create an index date for the untreated males that mitigates immortal time bias and ensures comparable person-time between groups given the absence of treatment exposure in the untreated group, a risk set sampling approach was employed to establish comparable index dates between groups [15, 16]. For every individual in the treated group, the duration (in days) from their RTT diagnosis to their first TROF initiation was calculated. A corresponding “risk set” of untreated individuals, defined as those with an RTT diagnosis who had not yet initiated TROF, was then identified. From this eligible pool, five untreated individuals were sampled for every one treated individual (1:5 ratio) and assigned a proxy index date equal to their own RTT diagnosis date plus the treated individual’s specific diagnosis-to-treatment interval.
Fig. 1 Exclusion Criteria
Exclusion CriteriaFemales with RTT diagnosis were excluded. Individuals with < 6 months of continuous enrollment before and after their respective index dates were excluded to ensure adequate data were used for the analysis. Individuals with RTT with a history of cerebrovascular disease or brain trauma during any time prior to their RTT diagnosis were also excluded.
Study VariablesDemographics and Clinical Characteristics of Male Individuals with RTTIndividual patient and clinical characteristics were evaluated for both treated and untreated groups, beginning with the assessment of pre-index demographics, specifically age at the index date. Physician specialty (e.g., child neurology, clinical neurophysiology, etc.) was identified based on the provider who was seen closest to the index date among the two groups. To characterize the clinical journey of these patients, differential diagnoses (e.g., non-specific developmental delay [NSDD] and autism spectrum disorder [ASD]) were examined at any time prior to the index date. Additionally, the prevalence of clinical characteristics and comorbidities such as epilepsy, gastrostomy and RTT-related features such as loss of acquired communication skills, behavioral disorders were assessed during pre-index period and compared between the two groups.
Post-Index Treatment OutcomesTime to Non-PersistenceAmong the treated group, time to non-persistence was calculated based on the actual time on treatment. Persistence was defined as a treatment gap that is less than or equal to 90 days between TROF RXs while non-persistence was defined as a treatment gap of > 90 days between TROF RXs. Time to non-persistence was defined as the time from index date to the last TROF RX claim date. Among individuals who remained persistent through the end of follow-up, patients were censored at the last available follow-up date or the study end date, whichever occurred first. Among individuals who became non-persistent, the treatment end date was defined as the last claim date plus days of supply for the final TROF RX fill occurring before a treatment gap of > 90 days. Time to non-persistence, expressed in months, was calculated as: [(end of days’ supply after the last prescription fill − first prescription fill date + 1)/30].
Predictors of Non-PersistencePre-index (i.e., baseline) variables including comorbidities that may predict the likelihood of non-persistency among males treated with TROF (n = 51) during the 6 months follow-up were assessed using a two-step process. To alleviate the small sample of patients within each individual concomitant comorbidity and to generate a robust model, we grouped the list of individual pre-index clinical comorbidities into clinically relevant categories and operationalized these as binary indicators based on the presence of ≥ 1 diagnostic claim. The list of individual comorbidities within the respective major categories is presented in Supplementary Table 1. To examine the individual effect of the potential predictors of non-persistence, unadjusted univariate logistic regression models were first used to evaluate the association between each predictor and non-persistence. As a second step, a multivariable logistic regression, adjusted for clinical meaningful predictors (chosen a priori), assessed the combined effect of the individual predictors of treatment non-persistence.
Statistical MethodsDescriptive statistics were used to summarize pre-index characteristics and treatment outcomes. Categorical variables (e.g., physician specialty, comorbidities etc.) were reported as frequencies and percentages. Continuous variables (e.g., age) were summarized using means and standard deviations (SD), as well as medians and interquartile range (IQR). For the cohort of males in the TROF-treated group, the duration of therapy was assessed using Kaplan–Meier analysis, with time to non-persistence expressed in months. As mentioned above, univariate and multivariable logistic regression models were conducted to assess the magnitude of association between pre-index predictors and non-persistence during 6 months of follow-up. As a result of small sample size, a simple model with limited covariates was prioritized in the adjusted model, which included adjusting for age and the four broad clinically meaningful comorbidity categories (i.e. gastrointestinal, infectious, respiratory, and neurological disorders) which were included as covariates in the multivariable logistic regression analyses. Model stability was evaluated by sequentially adding covariates to assess the consistency of estimates.
Results of the multivariable logistic regression models were reported as odds ratios (ORs) and 95% confidence intervals (CIs), with a statistical significance at a p value of < 0.05. All statistical analysis was conducted using Anlitiks proprietary RapidAnalyzer™ analytic platform that is powered by SQL and RStudio.
Comments (0)