Data Sources
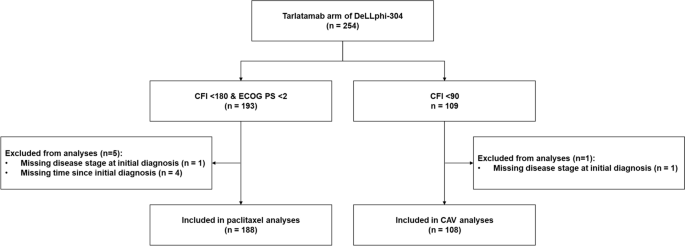
The analyses leveraged individual-level patient data (IPD) on tarlatamab (DeLLphi-304 trial; NCT05740566) collected from patients who were enrolled between May 2023 and July 2024 and assessed up to the primary analysis data cut-off (January 2025). Published aggregate-level data (AgD) was used for paclitaxel (Owonikoko 2020; NCT02038647) and CAV (GFPC 0501; NCT00418743) [10, 11]. Owonikoko 2020 was a phase II randomized controlled trial that enrolled patients with platinum-refractory ES-SCLC [chemotherapy-free interval (CFI) < 180 days] in North America and Europe between May 2014 and October 2015 to receive either alisertib plus paclitaxel or placebo plus paclitaxel [11]. GFPC 0501 was a phase II randomized controlled trial conducted in France between December 2009 and June 2011, comparing CAV with oral chemotherapy in platinum-refractory ES-SCLC (CFI < 90 days) [10]. Only AgD from the paclitaxel plus placebo (referred to hereafter as paclitaxel) arm in Owonikoko 2020 and the CAV arm in GFPC 0501 were used in the analyses.
All three trials enrolled individuals with platinum-refractory or platinum-resistant ES-SCLC and were restricted to individuals who did not have symptomatic CNS metastases, had adequate laboratory values, and had no major comorbidities. To facilitate cross-trial comparisons and to account for differences in the CFI threshold used to define platinum-resistant disease, the DeLLphi-304 trial IPD was restricted to align with key eligibility criteria of the comparator trials. Specifically, the IPD from the tarlatamab arm of the DeLLphi-304 trial was restricted to individuals with platinum-refractory disease or a CFI < 180 days and who also had an Eastern Cooperative Oncology Group Performance Score (ECOG PS) < 2 for the paclitaxel comparisons, and to individuals with platinum-refractory disease or a CFI < 90 days for the CAV comparisons.
This study involved use of de-identified data from DeLLphi-304 and previously published aggregate-level summary statistics from Owonikoko 2020 and GFPC 0501, compliant with the United States (US) Health Insurance Portability and Accountability Act (HIPAA) and the Helsinki Declaration of 1964 and its later amendments or comparable ethical standards. The US Department of Health and Human Services does not consider analysis of de-identified secondary data to meet the definition for human subject research. Therefore, this study was exempt from federal regulations and did not require patient consent or institutional review board approval.
Selection of Baseline Variables for Adjustment
The covariates included in the MAIC were chosen a priori based on a multi-step process which included a review of prior literature, physician interviews, multivariable regression analyses using data from the DeLLphi-301 trial, meta-regression analysis of patient characteristics and outcomes from published clinical studies, and clinical evaluation [17]. The following covariates were identified as relevant prognostic factors or potential effect modifiers for the MAIC analyses and were used in previous studies: age, sex, race, smoking status, ECOG PS, disease stage at initial diagnosis, CFI, brain metastases, liver metastases, and time since initial diagnosis [17,18,19,20,21].
The MAIC analyses adjusted for differences in all available prognostic factors and effect modifiers that were reported in the comparator trials. The comparisons with paclitaxel were adjusted for age, sex, smoking history, time since initial diagnosis, ECOG PS, disease stage at initial diagnosis, brain metastasis, and CFI. The comparisons with CAV were adjusted for age, sex, ECOG PS, and disease stage at initial diagnosis. Due to the lack of reporting in the comparator trials, adjustments could not be made for race or liver metastasis in the paclitaxel analyses, and for race, smoking history, brain metastases, liver metastasis, or time since initial diagnosis in the CAV analyses. Individuals enrolled in the DeLLphi-304 trial who were missing relevant baseline covariate information were excluded from the analyses.
Study Endpoints
Outcomes of interest included OS, PFS, ORR, and disease control rate (DCR). The analyses leveraged data from the intention-to-treat population of each trial (e.g., individuals who did not have an evaluable tumor response were included in the denominator of the ORR and DCR calculations). The definitions of these outcomes were similar between the three trials, with OS defined as the time from randomization until death from any cause, PFS defined as the time from randomization to disease progression or death from any cause, ORR defined as the percentage of patients who achieved a partial response or complete response, and DCR defined as the percentage of patients who achieved a partial response, complete response, or stable disease. All trials assessed tumor response according to the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1) criteria. The AgD on outcomes for the comparator trials was extracted from the primary publications, specifically, Fig. 1C (OS), Fig. 1A (PFS), and Table 2 (ORR and DOR) reported in Owonikoko 2020 and Fig. 1 (OS), Fig. 2 (PFS), and Table 5 (ORR and DCR) reported in GFPC-0501 [10, 11].
Statistical Methods
The analyses leveraged IPD from the tarlatamab arm of DeLLphi-304 trial and published AgD for the paclitaxel arm of Owonikoko 2020 and the CAV arm of GFPC 0501 [10, 11, 14]. For OS and PFS, the published Kaplan–Meier (KM) curves from the comparator trials were digitized using WebPlotDigitizer to convert the KM curve figures from the study publications into numeric values for the time points and corresponding survival probabilities [22]. The digitized data were then used to simulate pseudo-IPD for each KM curve using the validated algorithm by Guyot 2012 [23]. The accuracy of the digitization was assessed by comparing the summary statistics from the pseudo-IPD against the published results from the comparator trials.
Due to the lack of a common comparator arm, an unanchored MAIC was conducted to estimate the comparative efficacy of tarlatamab relative to paclitaxel and relative to CAV after adjusting for imbalances in the distribution of baseline effect modifiers and prognostic factors. Within the MAIC analyses, balancing weights were derived such that the average baseline characteristics of the weighted DeLLphi-304 trial matched the published aggregate-level baseline characteristics of the comparator trial. Given the limited sample sizes of the trials, only the mean values of continuous covariates were controlled for in the main analyses as opposed to both means and standard deviations.
For the paclitaxel comparisons, Owonikoko 2020 did not directly report the mean and instead reported the median (range) for age and time since initial diagnosis. Within the paclitaxel analyses, age was modeled as a continuous covariate whereby the reported median value was used as an approximation of the mean under the assumption that this variable was symmetrically distributed. In contrast, the reported median value for time since initial diagnosis could not be used as a reasonable approximation of the mean because this variable was likely to be right skewed. To address this issue, time since initial diagnosis was modeled as a binary covariate whereby the reported median value of the comparator trial was used as a cut-point to create a binary variable in which 50% of the Owonikoko 2020 trial population would be above the median and 50% would be below the median.
To evaluate the impact of reweighting on the sample size, the effective sample size (ESS) was calculated as \(_\right)}^/\left(\sum _^\right)\) where \(_\) is the estimated weight for the \(^\) individual [24]. To assess the effectiveness of matching in minimizing differences between study populations, standardized mean differences (SMDs) were calculated before and after weighting [25]. To facilitate the estimation of the SMDs, standard deviations were imputed based on the reported range using the method described in Walter and Yao (2007), where necessary [26]. The distribution of the rescaled weights was examined to identify the presence of extreme weights.
A weighted Cox proportional hazards regression model was used to estimate HRs for OS and PFS and a weighted logistic regression model was used to estimate odds ratios (ORs) for ORR and DCR. In addition, weighted Kaplan–Meier curves and risk tables were presented for the OS and PFS analyses. To account for uncertainty in the derivation of the weights, robust variance estimation was used to estimate the 95% CIs.
E values were calculated to provide the minimum strength of association that an unmeasured confounder would need to have with both the treatment and outcome to fully explain away the observed magnitude of effect. [27]. Larger E values (typically greater than 2 or 3) suggest that a substantial degree of unmeasured confounding would be required to fully account for the observed effect estimate.
For the OS and PFS analyses, the proportional hazards assumption was evaluated based on an examination of Schoenfeld residual and log cumulative hazard plots. In instances where there was evidence of a potential violation of this assumption, the difference in the restricted mean survival time (RMST) was assessed [28]. The 95% CI for the RMST in the unweighted (unadjusted) analyses were estimated using the method described in Conner et al. (2019) [29]. To account for uncertainty in the estimation of the weights in the MAIC-weighted (adjusted) analyses, the 95% CIs for the RMST estimates were estimated using the bootstrap percentile method with 10,000 iterations.
Sensitivity analyses were performed to assess the robustness of the findings. For both the paclitaxel and CAV analyses, a sensitivity analysis was conducted in which we did not control for covariates that were already balanced between trials (i.e., SMD ≤ 0.1) or for disease stage at initial diagnosis [since information of ES vs. LS was not directly available in the DeLLphi-304 trial and was approximated using the American Joint Committee on Cancer (AJCC) tumor-node-metastasis (TNM) stage]. For the paclitaxel analyses, a second sensitivity analysis was conducted by treating time since initial diagnosis as a continuous variable whereby the reported median value was used as an approximation of the mean. For the CAV analyses, a second sensitivity analysis was conducted in which both the mean and standard deviation of age were controlled for since both values were directly reported in GFPC 0501. Further adjustment for the standard deviations of continuous baseline covariates in the paclitaxel comparisons was not explored because the standard deviations was not reported in Owonikoko 2020. Finally, a third sensitivity analysis was conducted for both the paclitaxel and CAV comparisons using an updated data cutoff of DeLLphi-304 (April 29, 2025).
The MAIC analyses were conducted in accordance with guidance from the EU JCA [30] and the National Institute for Health and Care Excellence Data Support Unit Technical Support Document 18 (NICE DSU TSD 18) [24]. The study did not require patient consent or ethics committee review due to the use of de-identified, secondary data. Statistical analyses were conducted in R (version 4.4.2) and R codes were based on those published by the NICE DSU TSD 18 [24].




Comments (0)