
Remember me



This study focused on the potential environmental value of patient self-care in the UK by evaluating the potential impact on GHG emissions of the substitution of all self-treatable healthcare visits by over-the-counter (OTC) and self-care medication. Ethics approval was not required for this study, which did not involve any animals or human participants. The potential and current impact on GHG emissions of self-care medication was also explored for allergic rhinitis, with the example of fexofenadine, a second-generation antihistamine medication which is available without a prescription in the UK and has demonstrated efficacy, with associated improvements in quality of life [17]. Equivalent doses of prescription and OTC preparations of fexofenadine have equivalent potency, although prescribed preparations can include a higher dose level than OTC products. The impact was measured in terms of patient care pathway GHG emissions only, based on a modelled reduction in HCRU (primary care [PC] and accident and emergency [A&E] use) [6]. The study compared a prescription-based journey with a self-care journey and therefore includes only the use phase, with no analysis of the carbon footprint associated with the product material acquisition and pre-processing production, distribution and storage, and end of life as per the GHG protocol [18, 19].
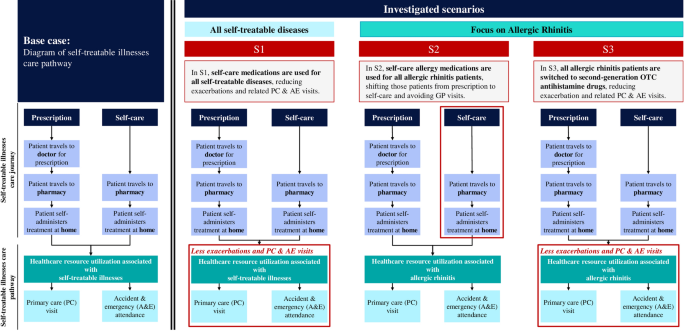
Patient Care Pathway (PCP)In line with the technical guidance from the Sustainable Healthcare Coalition on sustainable patient care pathway analysis, the impact on HCRU of self-managed cases was measured through three outcomes: PC consultations, A&E attendance, and patient travel [20]. Among other possible outcomes, inpatient admission and surgery were excluded as these are not applicable to self-treatable conditions. An approach was applied which mapped HCRU associated with self-treatable illnesses for pathways with and without a visit to the doctor for a prescription (the only difference between the prescription and self-care pathways is the presence of this visit for the former) (Fig. 1) and estimated carbon emissions from the resulting PCP.
Fig. 1
Diagram of self-treatable illnesses care pathway: base case and investigated scenarios. A&E accident and emergency, PC primary care, S1 scenario 1, S2 scenario 2, S3 scenario 3
General AssumptionsThe study used emission factors from the NHS estimated in Tennison et al. following a top-down approach which assumes an extended definition of the GHG protocol including patient and visitor travel [21]. The carbon footprint was estimated for HCRU for self-treatable healthcare utilisation and the avoidable emissions if the amount of OTC sold today were instead obtained via prescription for all self-treatable diseases and for allergic rhinitis alone. NHS GHG unitary emission factors were applied to HCRU to measure the associated GHG emissions of different scenarios of self-care adoption for all self-treatable conditions, and more specifically in the field of allergies.
Emissions FactorsTwo sources, Tennison et al. [21] and the Sustainable Healthcare Coalition [22], were identified from the literature as the most representative and up-to-date sources for NHS England emission factors. The dataset reported by Tennison et al. was selected as it provides the most recent NHS England unit emission estimates derived from the 2019 NHS carbon footprint. These estimates encompass direct emissions from sources owned or controlled by healthcare organisations, indirect emissions associated with purchased energy consumption, broader value-chain emissions linked to organisational activities, as well as emissions generated through the transportation of patients and visitors. Accordingly, this source was selected for use here [21]. The analysis incorporated the following healthcare event-specific estimates reported by Tennison et al.: 66 kg CO2eq per primary care visit and 75 kg CO2eq per A&E visit [21]. In the absence of equivalent data for Scotland, Wales, and Northern Ireland, these figures were used universally [23,24,25].
Anaesthetic gases and metered dose inhalers as well as visitor travel were removed from the emission factor as these were not applicable to our study. Where relevant, patient travel was recalculated to be specific for travel to pharmacies in the UK.
Scenarios and Modelling ApproachThree investigated scenarios were included in the analysis and are described below. For each scenario we compare to the base case (i.e. the situation today) and only look at incremental GHG emission savings that can be achieved. The base case and the three investigated scenarios are presented in Fig. 1, and the scenarios are described below.
Scenario 1 (S1) was used to indicate the environmental value of self-care. This scenario assumed that self-care medications were used for all self-treatable diseases, including not only allergies but also headache, colds, indigestion, and other commonly self-treated conditions, and provided the total GHG emissions that would be saved if all self-treatable diseases were treated with OTC medication and all HCRU (GP and A&E visits) were thereby avoided. The number of GP and A&E visits that would be avoided (from published data [6]) was multiplied by the emissions factors as described above to obtain the total emissions avoided per person.
Scenario 2 (S2) focused on allergic rhinitis (i.e. the priority indication for this work) and evaluated the share of allergy medications that are currently sold with a prescription, and the environmental impact in terms of reduced GP visits if all prescription were replaced by OTC medication. The number of prescriptions for allergic rhinitis was multiplied by the emissions factors as described above to obtain the total emissions avoided per person.
Scenario 3 (S3) measured the impact of switching all patients with allergic rhinitis on prescribed medication to second-generation OTC antihistamine drugs (fexofenadine) to evaluate the reduction on HCRU (GP visits) in the event of severe allergy episodes. The avoided HCRU (from published data [6]) was multiplied by the emissions factors as described above to obtain the total emissions avoided per person.
For each scenario, the total emissions avoided per person was multiplied by the total patient pool to derive the total GHG emissions that would be avoided. A schematic overview of the modelling approach is presented in Fig. 2.
Fig. 2
Schematic overview of the modelling approach. A&E accident and emergency, GHG greenhouse gas, GP general practitioner, HCRU healthcare resource utilisation, S1 scenario 1, S2 scenario 2, S3 scenario 3
Data InputsFor S1, HCRU attributable to self-treatable illnesses was directly available in the literature based on a study that estimated the socio-economic impact of self-care in the UK [6]. For S2, 2023 market data on OTC sales of allergy medication were used to derive the number of PC visits avoided. An estimated 1.4 packs of allergy medication per OTC trip was found, with one or two trips per buyer. The range 1.4 to 2.8 was therefore taken as an upper and a lower boundary. The total number of OTC boxes was divided by 1.4 and 2.8 to estimate the number of PC visits required to prescribe an equivalent amount of allergy medication. The same logic was applied to S3, with market data on allergy drugs delivered upon prescription being used. Yet, as only a proportion of patients would feel comfortable to self-manage their allergy symptoms, an adjustment factor was used, based on a behavioural study conducted in the UK in which it was found that 58% of people would be comfortable self-treating allergies [26].
Table 1 summarises the impact on HCRU in terms of PC visits for S1 (25–48 million) [6], S2 (14–29 million), and S3 (8–15 million) [21, 26,27,28,29,30]; additionally, 5–10 million A&E visits are associated with S1 (none assumed for S2 and S3) [6].
Table 1 Healthcare utilisation modelled for scenarios 1–3Expert ReviewMeetings were held between February 2024 and May 2024 with two subject matter experts to review the methodology, audit the GHG emission impact model, assess the data sources used, and discuss the findings of the study. Any disagreements were fully discussed and resolved at online meetings during this timeframe.
Comments (0)