This descriptive survey provides an overview of real-world management and unmet needs of patients with LACC in China. It underscores the high disease burden, specific deficiencies in treatment patterns, accessibility, and physician awareness, highlighting the need for targeted interventions. Despite the availability of clinical guidelines for LACC, the heterogenous nature of this cancer complicates clinical decision-making. As new treatments emerge, there will be an even greater need to identify tailored treatment strategies based on a deeper understanding of patient characteristics, differences in disease course, and disparities in medical resources. Furthermore, initiatives to improve access to guideline-concordant concurrent CRT as a definitive treatment for LACC in China remain imperative.
In this study, a high proportion of patients (67.7%) had LACC (FIGO 2018 stage IB3–IVA) reported, emphasizing the importance of screening, early diagnosis, and timely treatment. However, a standardized definition of LACC is lacking in current Chinese clinical practice, likely due to inconsistencies across guidelines. SGO and ESGO guidelines define LACC as stages IB3 and IIA2-IVA [5, 6], while NCCN guidelines lack definitions for common pathological types of LACC. Chinese guidelines adopt a narrower definition of LACC as stages IB3 and IIA2, and define IIB–IVA as mid-to-late stage [8, 9].
Additionally, non-standardized staging can adversely affect clinical decision-making. A large-scale Chinese study reported that 35.7% of CC cases had non-standardized clinical staging based on FIGO criteria, including missing, incomplete, incongruous, or vague staging descriptions [15]. Addressing these challenges requires implementing a standardized LACC definition within Chinese guidelines and enhancing physician education to improve diagnostic accuracy, and enable clear, standardized staging.
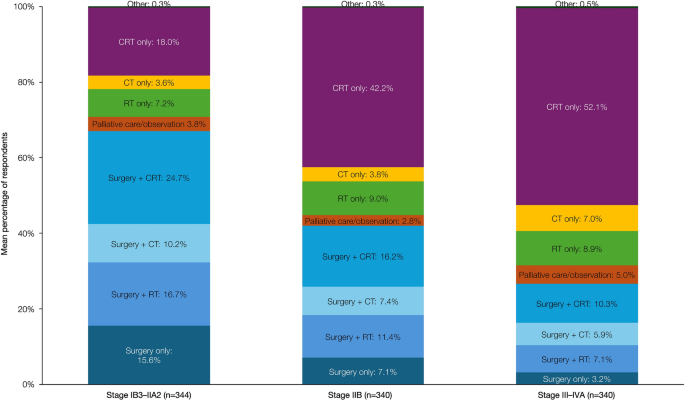
Despite high proportions of physicians regarding guidelines as highly important treatment decision drivers, the use of surgery-based treatments was high (26.6–67.1%) and there was low adoption of CRT alone (18.1–52.1%), practices inconsistent with guideline recommendations of definitive concurrent CRT as the preferred standard of care for LACC [7,8,9], highlighting a significant implementation gap between guideline recommendations and actual clinical practice in China.
This discrepancy may stem from several interrelated factors. First, the lack of RT (especially BT) equipment and specialized RT physicians is notable and reflected in this study. Only 63.9% of physicians had access to both EBRT and BT; 6.7% of physicians reported no RT facilities in their hospitals, and 18.9% reported that only EBRT was available. Among patients with LACC undergoing concurrent CRT in this study, EBRT plus BT was the most commonly used form of RT; however, this was only reported in 57.7%, revealing a large implementation gap to the guideline recommendations [16]. China has one of the highest estimated RT demands, with a shortage of experienced and qualified specialists, a need for high-quality EBRT and BT, and presenting challenges in training personnel [17]. Initiatives to improve availability of RT equipment, expertise, and training are clearly needed.
Second, this challenge is compounded by the high cost of concurrent CRT. Despite overall health insurance coverage being high in this study (82.3%), the fact that most respondents reported RT to be reimbursed by insurance should not be interpreted as full coverage or the absence of out-of-pocket payments. In China, reimbursement typically reflects partial coverage rather than full payment; a nationwide multicenter study reported that medical insurance covered only around 43–55% of direct medical costs for CC, and catastrophic health expenditures remained common, particularly among patients in rural areas due to differences in economic development [18]. Notably, some studies have found that surgery is less costly than RT or CRT [19, 20]. From our own experience, at Peking Union Medical College Hospital, the price of CC surgery over the past 2 years was ¥30,000–40,000 (US$4200–5600), while traditional RT cost approximately ¥50,000–80,000 (US$7000–11,200). If more advanced RT equipment such as intensity-modulated RT/volumetric modulated arc therapy is used, the price increases to around ¥100,000 US$14,000). Time costs with CRT, such as prolonged waiting periods (averaging 10.6 days in this study), and the requirement for frequent hospital visits over approximately 2 months, add to financial costs.
Third, for over 20 years, the only curative treatment options for LACC have been concurrent CRT and surgery, but evidence comparing these approaches remains equivocal. While large meta-analyses have shown no improvement in survival with concurrent CRT over surgery, with concurrent CRT offering superior DFS [24], others have shown a trend to overall survival (OS) superiority with concurrent CRT over surgery [HR 0.71 (95% CI, 0.49–1.02); probability of superiority, 96.9%] [25]. The present survey suggests that some Chinese clinicians believe that concurrent CRT does not offer a significant advantage over radical surgery. Radical surgery has emerged as a valid alternative for managing LACC in China and is recommended by the CSCO guidelines for patients with stages IB3 and IIA2 disease and limited access to RT [16], and Japanese guidelines include surgery as an option alongside concurrent CRT for patients with stage IIB CC [26]. Notably, FIGO guidelines recommend concurrent CRT for patients with stages IB3 and IIA2, but note that treatment modality should be determined based on resource availability and tumor- and patient-related factors, with neoadjuvant chemotherapy used if RT facilities are unavailable [27]. Collectively, tumor size alone is not the main obstacle for Chinese physicians to choose surgery-based treatments. Indeed, for specific pathological types that are less sensitive to RT and chemotherapy (such as small-cell neuroendocrine carcinoma of the cervix, clear cell carcinoma), surgery may improve the prognosis, especially in stages IB3-IIA2 [16, 28]. It is possible that surgical removal can reduce tumor burden, indirectly enhancing sensitivity to subsequent treatments, though evidence is lacking that debulking surgery is useful [29]. Treatment-related toxicity also influences clinical decision-making. Concurrent CRT is associated with higher rates of gastrointestinal toxicity and bone-marrow suppression than radical surgery alone [22], whereas surgery has been reported to have a significantly higher rate of major complications than concurrent CRT in later stages [23].
Importantly, our study found that most patients with LACC undergoing radical surgery required neoadjuvant or adjuvant CRT, RT, or chemotherapy. The accumulation of multiple treatment modalities increases complication risk, prolongs the treatment duration, and worsens patient quality of life [21]. It is clear that the decision between surgical management and CRT is guided by a range of clinical factors, and efforts should be made to reduce unnecessary treatment overlap, and ensure optimal therapeutic benefit. When addressing the complex challenges of CC, multidisciplinary team (MDT) collaboration leverages comprehensive strengths and has become an important model in clinical management [30]. In our study, clinical experience (which included personal and MDT experience) was reported as a key decision driver by 76.4% of respondents. However, MDT implementation remains incomplete and requires time to fully mature [31, 32].
Fourth, regarding physician and patient preferences, physicians might prefer surgery, as patients’ initial visits are usually with gynecology/gynecological oncology departments, where surgeons are more familiar with and confident in surgery. Patients might also prefer surgery, perceiving it to be a curative measure, and are likely to rely on their treating physician’s recommendations. Even with full knowledge of the risks, a notable proportion of patients still opt initially for surgery [33]. In China, regional inequality in education and heterogeneous economic development means that only about one-quarter of the adult population have basic health literacy [34], leading to a reliance on physician advice without full understanding. Indeed, our study found that 56.0% of patients had no treatment preference and relied on their physician’s recommendations, while 75.2% had full adherence to the prescribed regimens. The use of surgery is generally consistent with previous findings [14, 35], and underscores the need for enhanced physician education and greater patient awareness.
Beyond treatment selection, the quality and completeness of definitive concurrent CRT delivery remain critical determinants of outcomes in LACC. International guidelines recommend weekly cisplatin (or carboplatin if cisplatin-intolerant) as the standard concurrent chemotherapy backbone during definitive RT [5,6,7]. Guidelines also note that BT is a critical component of effective concurrent CRT, with image-guided techniques such as image-guided adaptive BT forming an increasingly important part of effective BT implementation [7, 36,37,38]. Prolonged overall treatment time (more than 56 days) is associated with inferior local control and survival [38,39,40,41,42]. In the present survey, however, to avoid excessive respondent burden, we did not collect granular information on specific technical components of concurrent CRT delivery. Nevertheless, certain patterns observed in this survey, such as the relatively frequent use of platinum-based doublet chemotherapy regimens during concurrent CRT, may serve as indirect signals of heterogeneity in concurrent CRT execution and underscore the need to further improve standardization and quality of concurrent CRT delivery in real-world practice.
Recent therapeutic advances further highlight the need for high-quality, standardized concurrent CRT as a foundation for treatment intensification. In the KEYNOTE-A18 trial, adding pembrolizumab to concurrent CRT significantly improved progression-free survival (PFS) and overall survival (OS) in patients with LACC compared with placebo plus concurrent CRT [hazard ratio (HR) for PFS, 0.72 (95% CI, 0.59–0.87); HR for OS, 0.73 (95% CI, 0.57–0.94) at the final analysis [43,44,45)]. The US FDA approved pembrolizumab plus concurrent CRT for patients with FIGO 2014 stage III–IVA CC in 2024. Chinese NMPA approval followed shortly afterwards for the same indication, based on the data from 112 patients with FIGO 2014 stage III–IVA disease in the Chinese cohort, which revealed a OS HR of 0.34 (95% CI, 0.12–0.95) and a PFS HR of 0.35 (95% CI, 0.16–0.74) [46]. Importantly, the regimen used in KEYNOTE-A18, now established as standard of care, requires high-quality, and standardized concurrent CRT, including EBRT followed by BT [44]; non-standard concurrent CRT may therefore limit benefits to patients from the latest treatment options [47].
This study had limitations. First, selection bias may have occurred, as respondents who were better informed and more interested were more likely to participate. Second, patient characteristics, treatment patterns, and healthcare resource use were reported by physicians, so recall biases might introduce measurement errors, although this is mitigated by the relatively large sample size. The data may have a hierarchical structure, with physicians nested within hospitals and city tiers, potentially underestimating errors. Finally, as the study only included physicians, it lacks the patient perspective, particularly regarding factors affecting patients’ adherence to treatment, preference, and unmet needs. Future research should include inclusive, co-designed studies to address this gap. Data on socioeconomic and demographic diversity (ethnic minority groups, rural vs. urban differences) were not collected, which may further limit the interpretability of the results.




Comments (0)