
Remember me
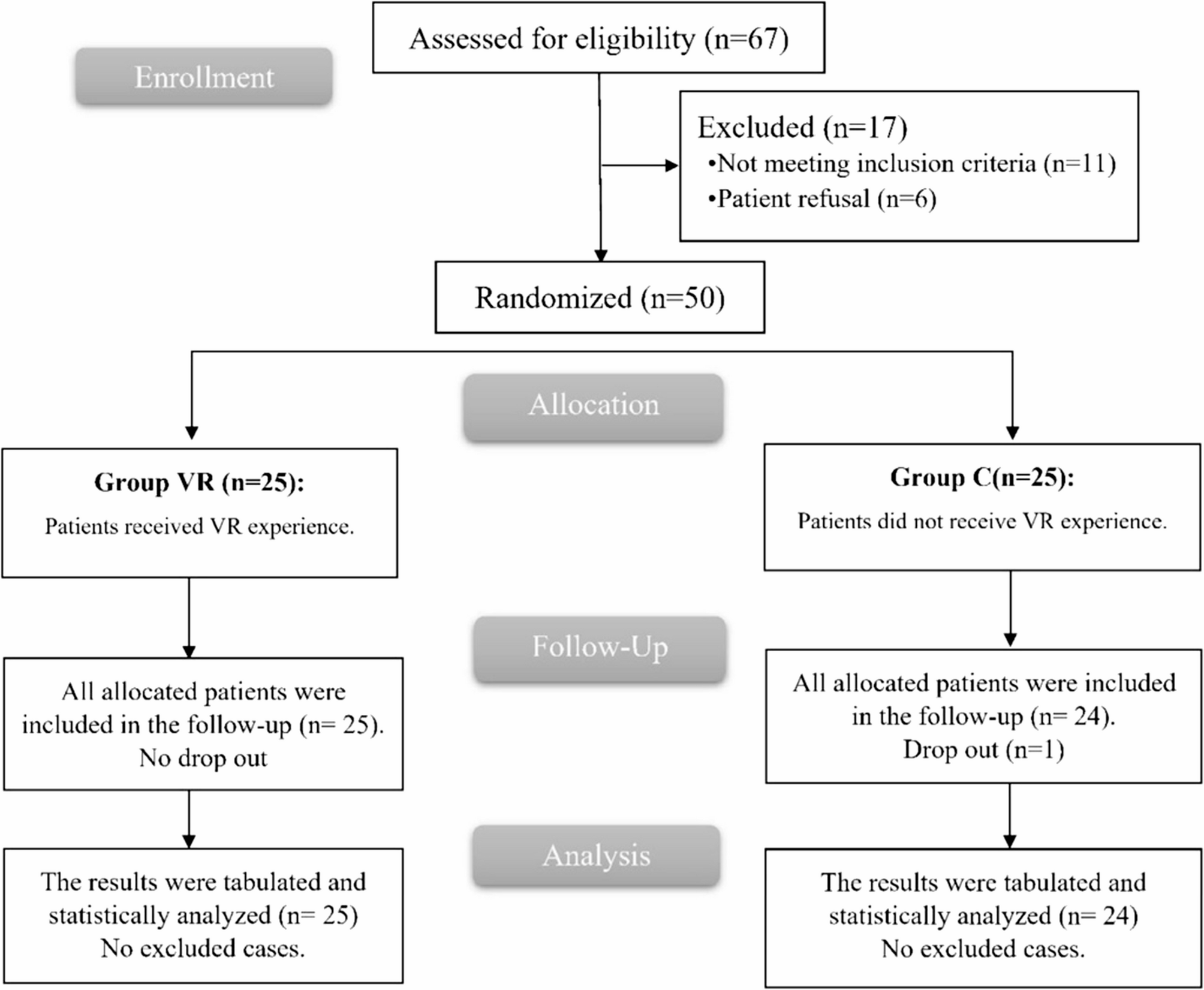
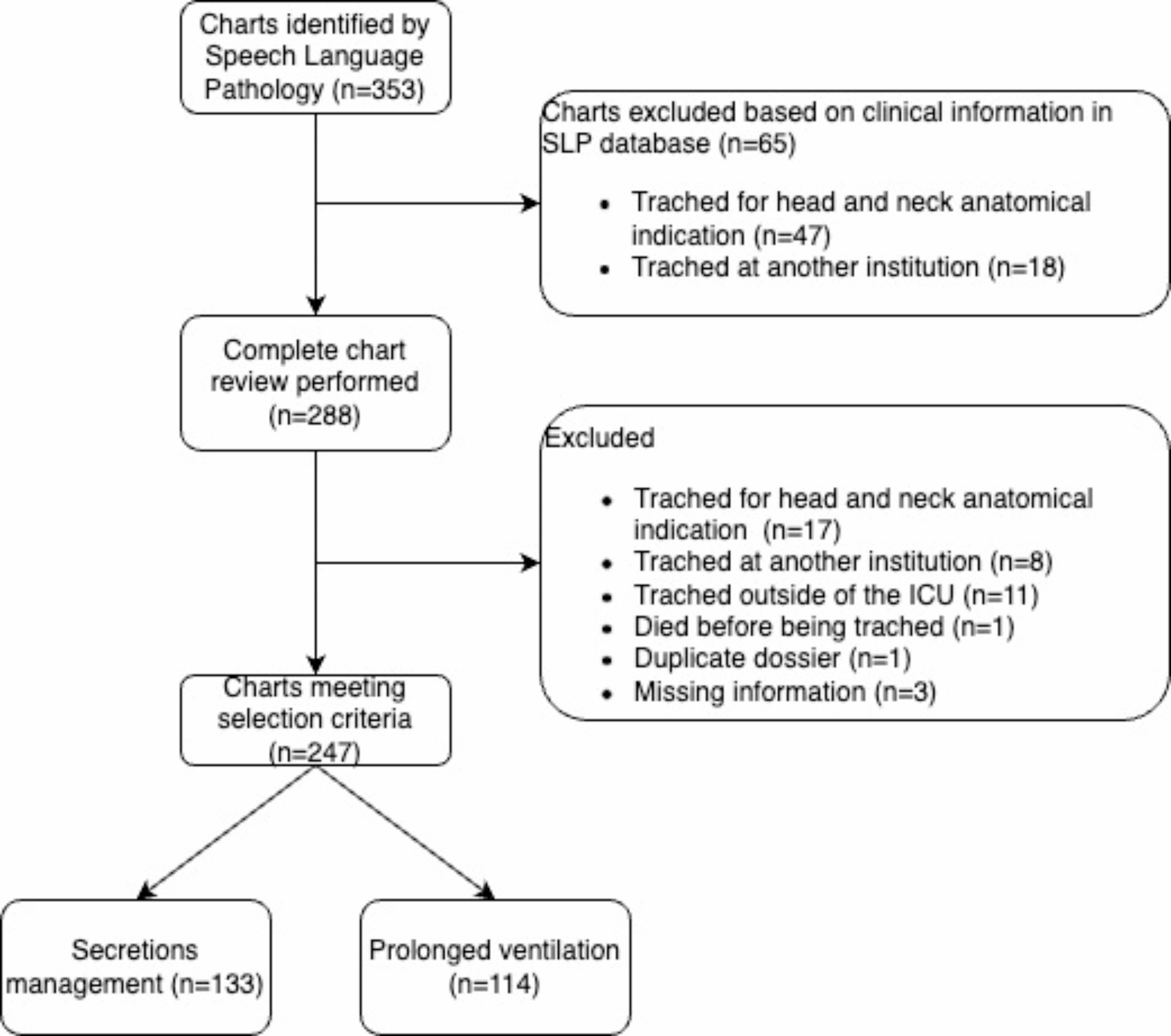
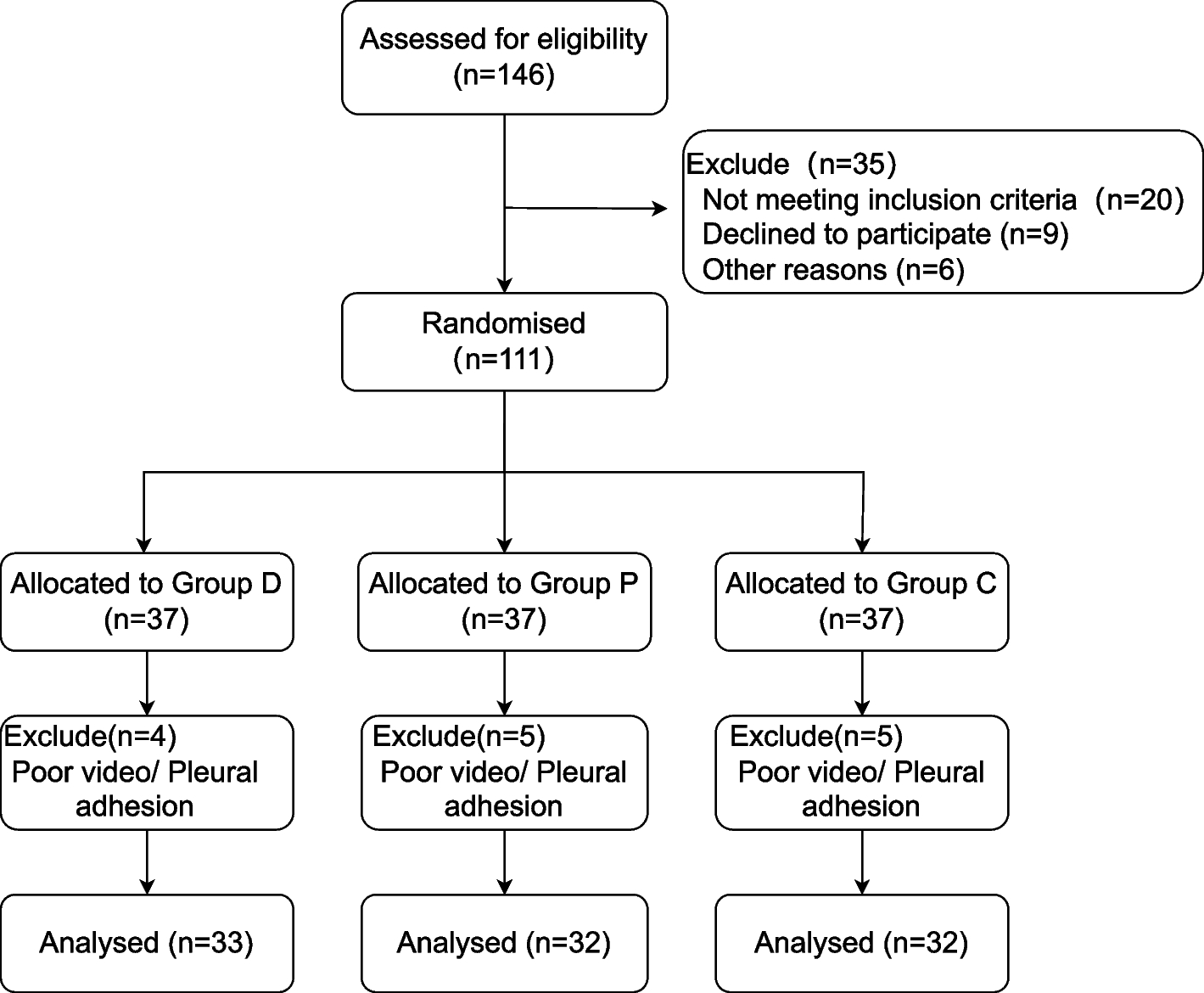
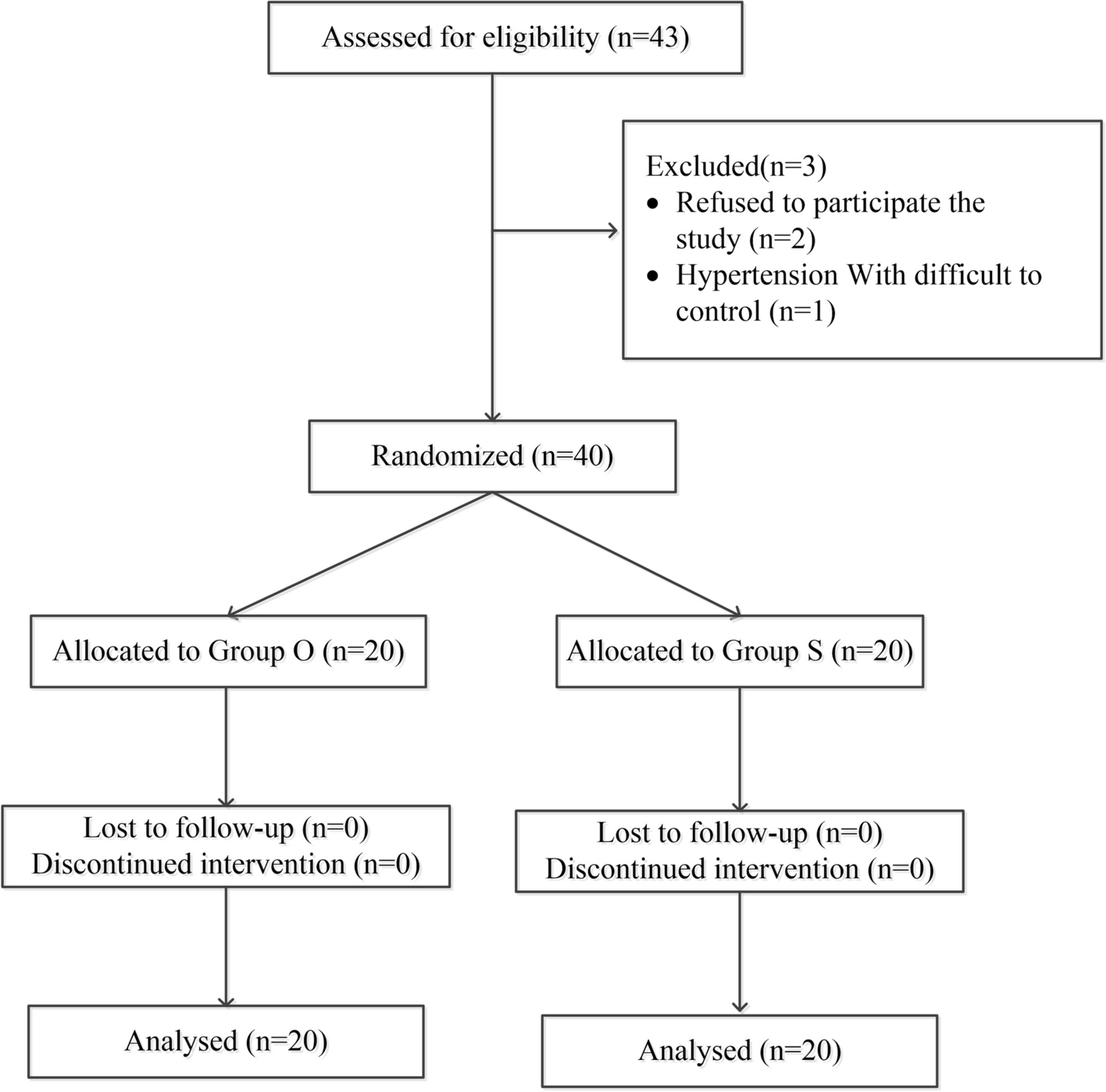
This prospective, randomised controlled clinical trial was approved by the Ethics Committee of Army Medical Center of PLA (approval number: Yiyanlunshen (2022) No. 188) and registered with the Chinese Clinical Trial Registry (registration number: ChiCTR2200062199). Data were collected from July 2022 to February 2023, and all enrolled patients signed an informed consent form. Patient enrolment and allocation were performed according to the study flowchart (Fig. 1).
Fig. 1 Inclusion and exclusion criteria
Inclusion and exclusion criteriaThe inclusion criteria for this study were as follows: (1) an American Society of Anaesthesiologists physical status (ASA) I or II; (2) aged between 18 and 65 years; (3) an FEV1 ≥ 70% of the predicted value and scheduled to undergo video-assisted thoracoscopic surgery requiring OLV. Patients were excluded from the study if they: (1) Patients with evidence of abnormal expiratory recoil (forced expiratory volume in 1 s < 70% of predicted value), chronic obstructive pulmonary disease or severe asthma, pneumothorax or thoracic closed drainage; (2) undergone thoracic surgery; (3) underwent a preoperative assessment indicating possible pleural adhesions, pulmonary bullae, etc.; (4) had a risk of lung contamination by blood or infectious secretions; (5) anticipated to have difficult airways.
Patients were randomly assigned to one of three groups using a random number table method: the control group (group C), the disconnection technique group (group D) and the preemptive OLV group (group P).
Preoperative preparations and anaesthesia protocolUpon arrival at the operating room, venous and arterial access was established, and the invasive arterial blood pressure (Edwards TruWave PX260), heart rate, blood oxygen saturation, and other basic vital signs were obtained. After denitrogenation for 5 min, anaesthesia was induced with 0.3–0.5 µg/kg of sufentanil, 0.03–0.05 mg/kg of midazolam, 0.2–0.3 mg/kg of etomidate, and 0.15–0.2 mg/kg of cisatracurium. The patients were intubated with a nonoperative lateral double-lumen tube (DLT). Commonly used pulmonary isolation tools include double-lumen endotracheal tubes and bronchial blocker, and there is insufficient evidence to show a difference in lung collapse [12]. Both have their own advantages, disadvantages, and indications, but in general, double-lumen tracheal catheters are often preferred because they can be inserted quickly, are less prone to displacement, and allow for the suctioning of secretions from either lung [13,14,15]. We therefore chose the double-lumen endotracheal tube as the lung isolation tool, the DLT was selected based on the preoperative chest CT scan, sex, and height [16]. The correct position of the tube was verified using a fibreoptic bronchoscope (FOB) both after intubation and after the patient was positioned. Anaesthesia was maintained with sevoflurane, propofol and remifentanil, as indicated by a BIS between 40 and 50. Cisatracurium was administered intermittently to maintain neuromuscular blockade. Perioperative blood pressure control is maintained within 20% above or below baseline blood pressure.Two-lung ventilation (TLV) was initiated using volume-controlled ventilation: the tidal volume was 6–8 ml/kg, the respiratory rate was 12 bpm, the I/E ratio was 1:2, the positive end-expiratory pressure was 5–10 cmH2O, and the fraction of inspired oxygen was 1.0. PetCO2 was maintained at 35–45 mmHg. Different strategies for OLV were implemented based on the various groupings. In group C, OLV was initiated when the surgeon commenced the skin incision and opened the lumen of the operative side. In Group D, OLV was initiated 2 min after disconnection of the DLT. This procedure started when the surgeon performed the skin incision. If the time to open the pleura exceeded 120 s or if the pulse oxygen saturation (SpO2) decreased from the previous level, the study was stopped, and the ventilator was connected immediately. In group P, OLV was initiated promptly after the patient was turned to the lateral position while the bronchial tube port was clamped on the operative side at the lateral position until pleural opening, The time between lateral position and pleural opening was recorded, which was guaranteed to be no less than six minutes. In OLV, the tidal volume was 4–6 ml/kg, the respiratory rate was 12–15 breaths/min, the PEEP was 5–10 cmH2O, the I/E ratio was 1:2, and the fraction of inspired oxygen was 1.0. PetCO2 was maintained at 35–45 mmHg. We did not utilize negative pressure suction to facilitate lung collapse because the optimal suction pressure suction pressure, suction time are not clear, and no studies have clearly established whether it can cause occult lung injury [3, 17, 18].
Lung collapse scoreVideos of the operative field were recorded during thoracoscopy after opening the pleura, and lung collapse scores were assessed by anaesthesiologist and thoracic surgeon who were blinded to the group allocation. The lung collapse scoring criteria included three main aspects [19]: space, colour, and surgeon satisfaction (Fig. 2). The lung collapse score is defined as the sum of the lung colour score, lung space score, and surgeon satisfaction score. Compared to other studies in which the satisfaction of lung collapse is solely determined at the discretion of the surgeon, our scoring criteria are more objective and accurate.
Fig. 2
Lung collapse scoring criteria details
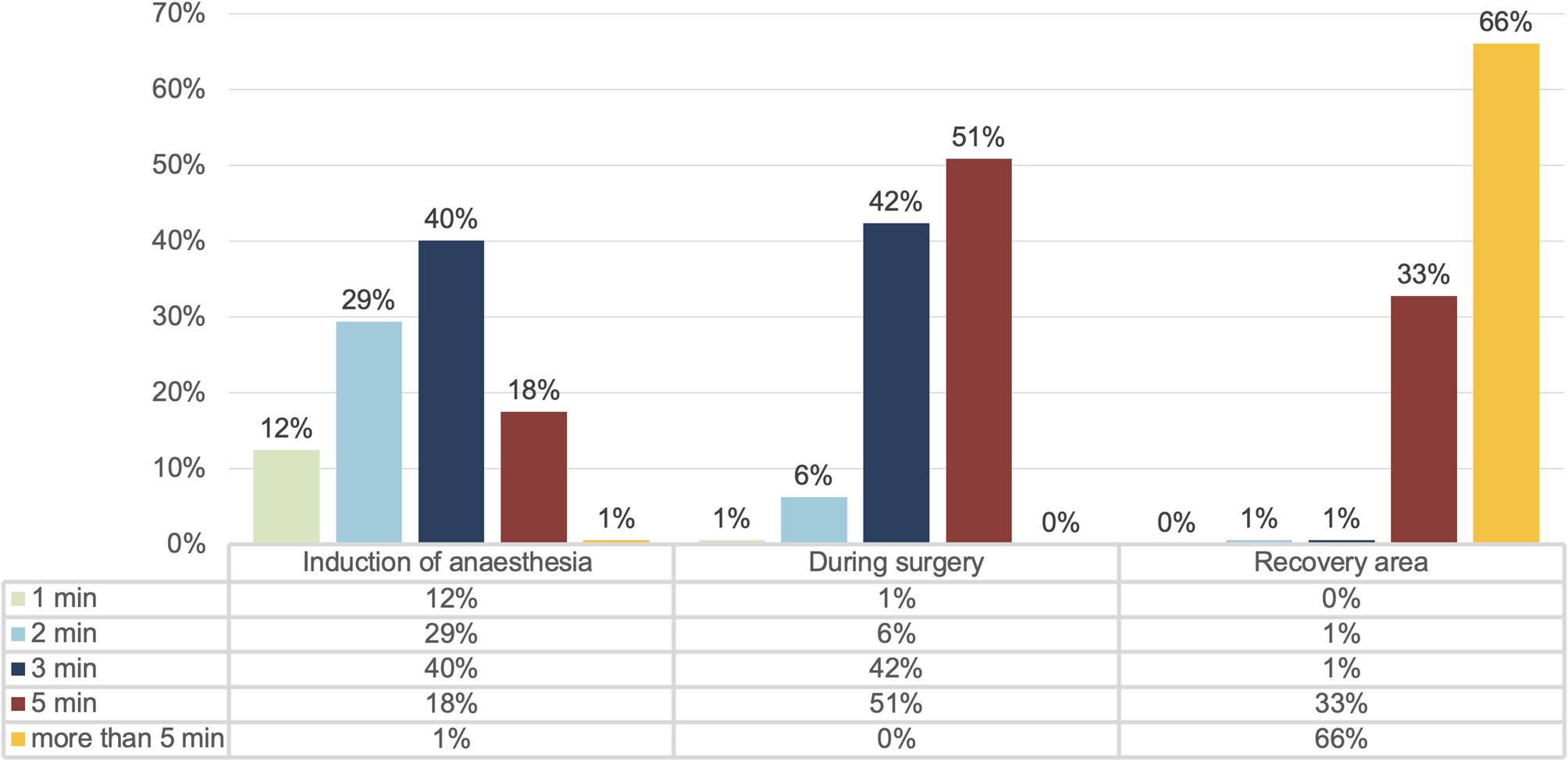
Outcomes measuresThe primary outcome was the time to satisfactory lung collapse, defined as the time required to reach a lung collapse score of eight points. The secondary outcomes included lung collapse scores at different time points (1 min, 5 min, 10 min, 15 min, 20 min, 25 min, and 30 min) after pleural incision; blood gas analysis at different time points (T1: preoxygenation state before the induction of anaesthesia, T2: 5 min after the start of OLV, T3: 15 min after the start of TLV, T4: 30 min after extubation); incidence rate of hypoxemia (SpO2 < 90%); basic operation-related information (Pleural opening times, OLV time) and the incidence rate of postoperative pulmonary complications (PPCs) within three days (the inclusion criteria were based on the 2015 European Perioperative Clinical Outcome standards [20]).
Statistical analysisThis study is a randomised controlled trial. Based on preliminary data, the time to satisfactory lung collapse was 14.56 ± 2.17 min in the D group, 13.92 ± 5.09 min in the P group, and 18.42 ± 3.26 min in the C group. Using PASS 15 software and one-way analysis of variance with a significance level of α = 0.05 and β = 0.10 and assuming a 1:1:1 ratio for the three groups and a 10% dropout rate, the calculated sample size required for each group was 32 participants. The normality of continuous variables was tested using the Shapiro‒Wilk normality test. The data were normally distributed, comparisons among the three groups were using one-way ANOVA, and intergroup analysis was performed using the Tukey's Honest Significant Difference test; the results are presented as the mean ± SD. The data were not normally distributed, comparisons among the three groups were using the Kruskal–Wallis test and intergroup analysis was performed using Bonferroni test, the results are presented as the median and interquartile range (IQR). Enumeration data are expressed as a percentage(%), and comparisons were made using Fisher's exact test.Statistical analyses were performed using SPSS version 27(IBM)and R Studio software version 4.3.3(R Project for Statistical Computing). All the statistical tests were two-sided, and a p value < 0.05 was considered to indicate statistical significance.
Comments (0)