Study design
This single-center, prospective, randomized intervention study was conducted at a tertiary hospital. The study was approved by the ethics committee of the Charité - Universitätsmedizin Berlin (Ethical Committee N° EA2/269/22 of May 2023) and at German Clinical Trials Register (DRKS00031785, date of registration 26.04.2023). Included patients gave their written informed consent. The study protocol was carried out in accordance with the Declaration of Helsinki and the CONSORT-Guidelines for randomized controlled trials.
Patients and setting
The trial was performed from the 11th of April 2023 and the 28th of June 2023. Adult patients (≥ 18 years) ASA physical status I–III who underwent elective surgery under general anesthesia with an LMA according to institutional standard operation procedures were checked for eligibility. Exclusion criteria included obesity (Body Mass Index, BMI > 30 kg/m²), cervical spine pathologies or restricted head rotation, contraindications to LMA use, and inability to provide consent.
Prior to inclusion, the cervical spine of the awake patient was evaluated for motion restriction, pain, and neurological pathology. Administration of anesthesia and performance of measurements were conducted in the anesthesia induction room of a central operating theater area. Induction of anesthesia was accomplished with the administration of intravenous opioids (fentanyl, sufentanil, and remifentanil) and propofol in accordance with the respective institutional standard operation procedures. Maintenance of anesthesia was carried out as total intravenous anesthesia (TIVA) or balanced anesthesia (sevoflurane). Depth of anesthesia was quantified through processed electroencephalography (Sedline®, Masimo Corporation, 52 Discovery Irvine, CA 92618, USA), and the study LMA was placed when the patient status index (PSI) was < 50. LMA type (cLMA: Ambu® AuraStraight™ vs. i-gel) was selected in adherence to the study protocol and prior randomization, and the size of the LMA was determined based on the specifications outlined by the manufacturer. Proper placement of the LMA was confirmed when a stable expiratory CO2 curve with values between 35 and 45 mmHg was observed and no detectable air was observed at a fresh gas flow (FGF) of 1 L/min. After LMA insertion a resting period of 5 min was allowed to equilibrate and warm the LMA before measurements began. Subsequently, adjustments were made to the ventilation settings and the cuff pressure of the cLMA was verified to be 60 cmH2O. The fraction of inspired oxygen (FiO₂) was set to 1.0 at an FGF of 3 L/min. The ventilation mode was set to pressure controlled. Inspiratory pressure (Pinsp, cmH2O), positive end-expiratory pressure (PEEP, cmH2O), and expiratory tidal volume (TV, ml) were recorded prior to measurement. Parameters were considered to be within the normal range if the Pinsp was less than 20 cmH2O at a PEEP of 3–5 cmH2O with a TV of 8 ml/kg body weight. These parameters were employed as a surrogate for adequate ventilation and correct positioning of both LMAs.
Primary Endpoint
The primary endpoint was OLP in cm H2O in head rotation at 60° left and right, without extension or inversion of the head. OLP was measured by closing the expiratory valve (APL valve, adjustable pressure-limiting valve) to 40 cmH2O, setting the FGF to 8 L/min and switching to manual ventilation mode without ventilating. This resulted in a steady state of the ventilation pressure (plateau in the ventilator graph). This numerical value was recorded as OLP by the anesthesia machine (Dräger Medical Primus®), the minimum detectable pressure step was 1 cmH2O. In addition, it was recorded whether an acoustic leakage of the LMA was perceptible at this time with one member of the study team listening for an audible noise over the mouth [14]. OLP was measured first at 0° and then at 60° head rotation, first to the left and then to the right, with no additional flexion or extension of the head.
All measurements were performed in the order mentioned above. After the initial OLP measurement was finished, the head was rotated, and we waited for the ventilation parameters to reach equilibrium. Once this occurred, the next OLP measurement was performed.
Secondary Endpoint
Secondary endpoints include the OLP in cmH2O at 0° head rotation and postoperative complications such as sore throat, hoarseness, swallowing difficulties, soft tissue damage (lip, tongue, oral and pharyngeal mucosa and larynx) and tooth damage on postoperative day 1. Tidal volume, Pinsp, and PEEP were measured before the start of the study measurements. Postoperative complications were assessed during a study visit on the first postoperative day and documented using our case report form.
Randomization
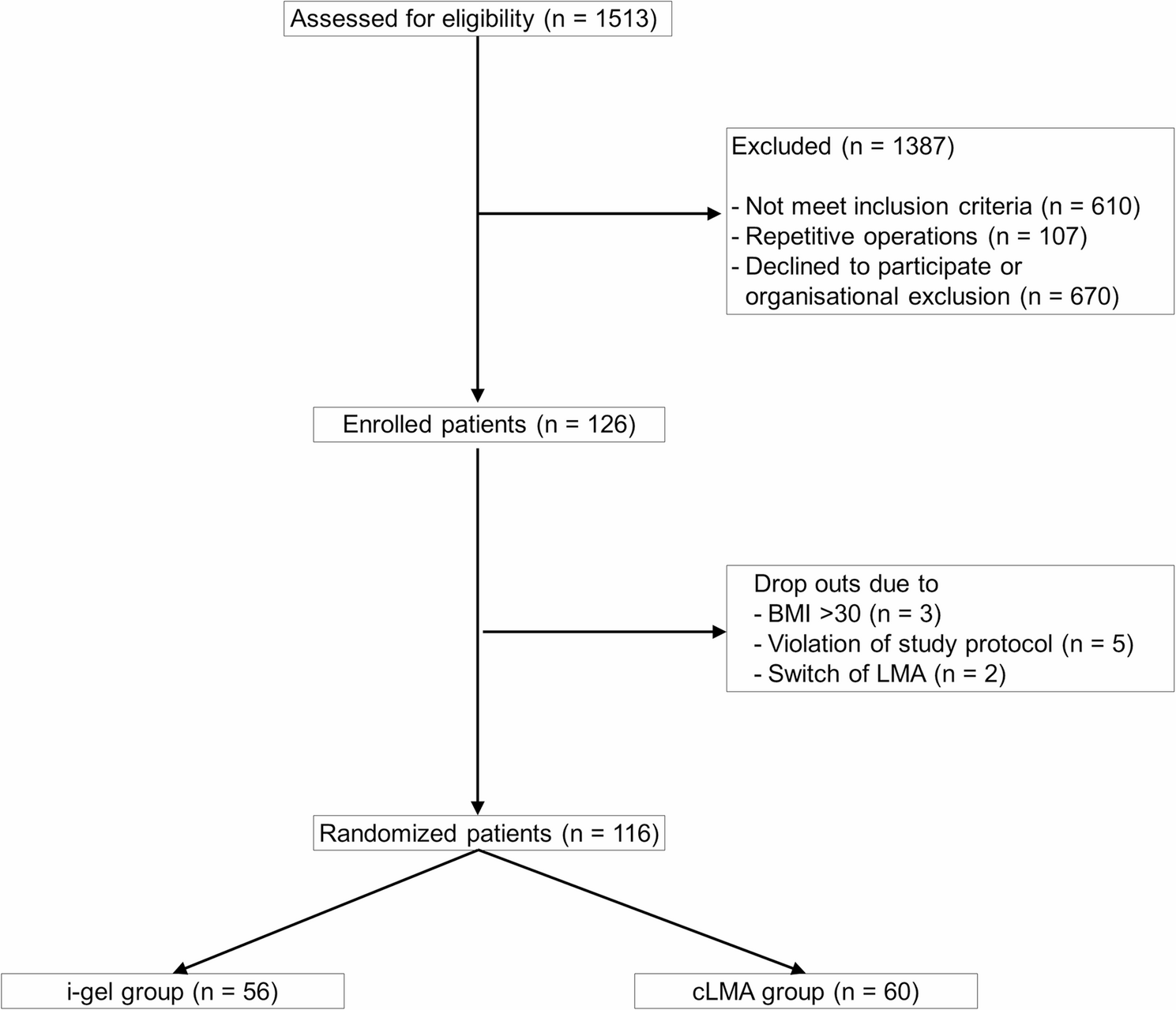
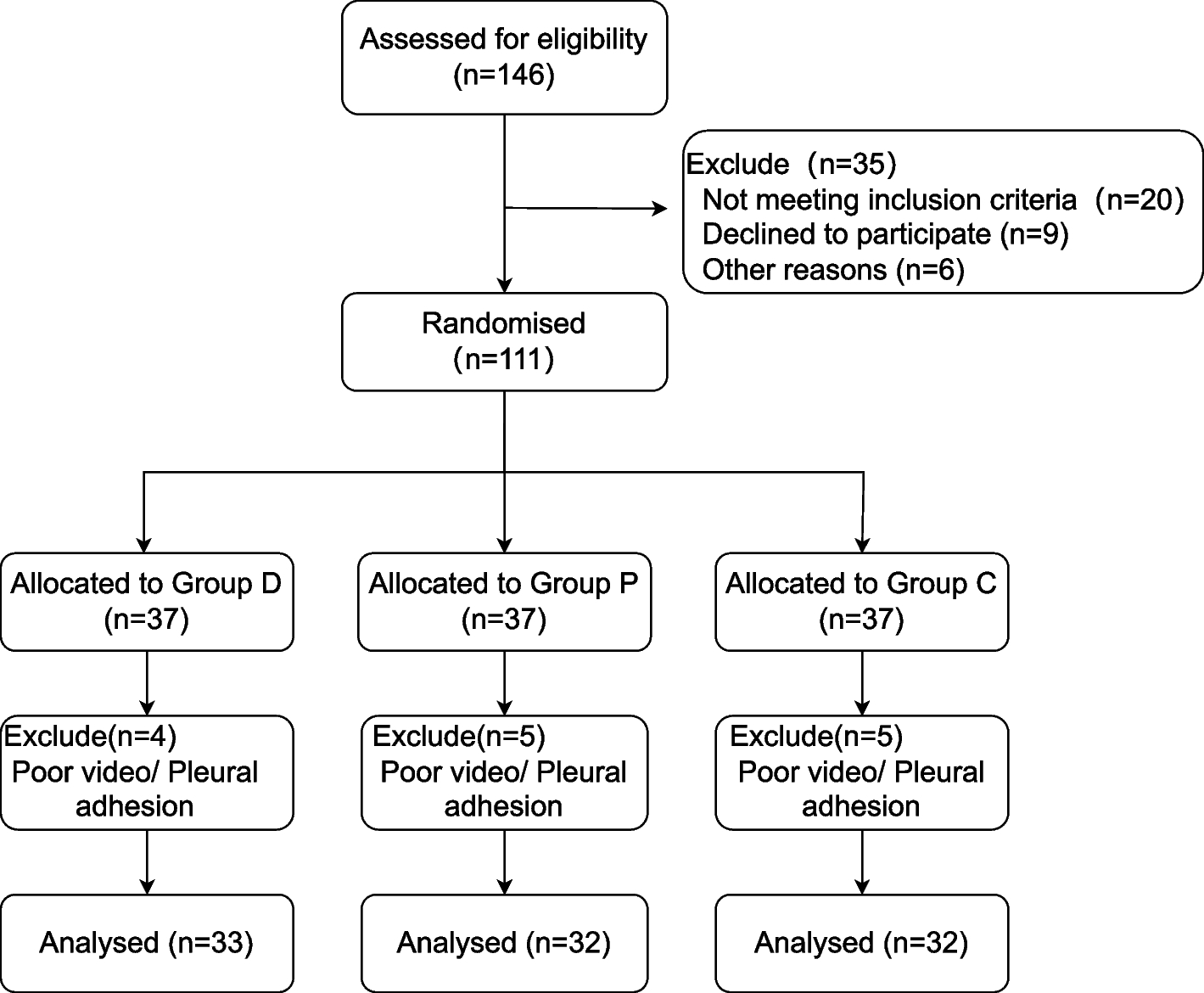
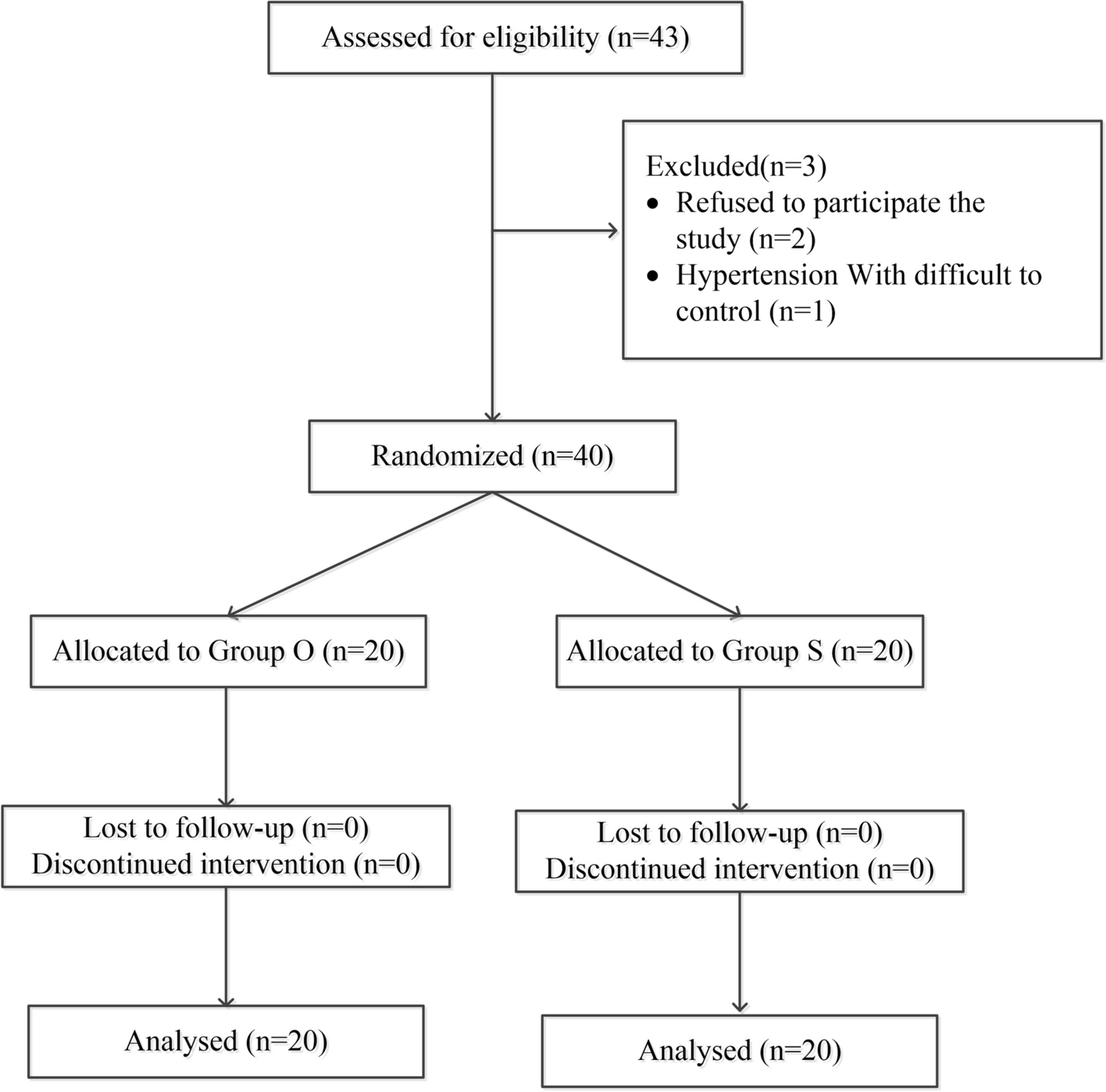
Patients were assigned to either cLMA or i-gel group in a 1:1 ratio using digital 4-block randomization. A sealed envelope was used for the allocation concealment method, which was opened by the study team after the patient was anaesthetized immediately before laryngeal mask insertion.
Sample size
We performed an a priori power analysis based on previous research [10, 12]. This showed a pooled standard deviation (SD) of 6.31327 for the difference between a laryngeal mask with cuff and an i-gel. A 3 cmH2O or greater difference in OLP was considered clinically relevant [10]. We calculated that a total sample of 114 patients would be needed to detect a significant difference between study groups for primary endpoint OLP (alpha-level of 5%, 1-β probability of 80%) [15]. To account for dropouts, a study design with a case number of 63:63 was planned.
Statistical methods
Data are reported as numbers of patients (%), median with 25 to 75th percentiles [IQR]. For univariate analyses of statistical significance, nominally scaled data were analyzed using chi-square test and ratio scaled data using Mann-Whitney test. Testing for normal distribution was carried out using the Shapiro-Wilk test. The level of statistical significance was set at P < 0.05. In general, the absence of a statistical difference does not imply formal equivalence.
Statistical analyses were performed with IBM SPSS Version 29.0.1.0; Armonk, New York, United States.

Comments (0)