
Remember me
The SBI’s EEG boot camp for anaesthesia was developed as part of the Safe Brain Initiative (SBI)—now an ESAIC research group—that focuses on to improving patient outcomes through patient-centred precision care (https://safebraininitiative.com/). Based on real-world evidence, SBI employs an advanced data-driven dashboard for continuous structured routine feedback to healthcare professionals. The core of the SBI is that posing the simple question ‘How are your patients doing after anaesthesia?’ can significantly improve patient care, as every clinician inherently strives to optimize quality of care. In this context, the EEG was identified as an essential tool to improve post-anaesthesia outcome. Hence, the SBI’s EEG boot camp for anaesthesia was founded in 2023 in Nykobing, Denmark. It has been iteratively developed and improved over several boot camps held in different locations, including Nykobing/Denmark (06–23), Glasgow/UK (10–23), Antalya/Turkiye (11–23), and Greifswald/Germany (12–23).
The course contents were derived from defined learning goals and then sorted into theoretical blocks that build on each other, concluding with a final block providing consolidation through practical training. In addition to theoretical and hands-on training, all learning is facilitated by providing all contents and learning goals in problem-based, algorithmic concepts (examples shown in supplement 1). With the algorithms, the participants receive clearly defined clinical strategies that they can directly incorporate into daily practice. Furthermore, learning consolidation is supported through online-based quiz rounds after each block as well as by actively abstracting the knowledge by transferring it from cases in the operating room to the intensive care unit (ICU).
Learning goalsTo define the contents for the SBI’s EEG boot camp for anaesthesia we first defined what knowledge we consider essential to leverage the full potential of EEG monitors. To provide motivation for using EEG monitors at all, users are required (1) to know and understand how EEG monitoring can contribute to improving patient outcomes. To enable users to actually perform EEG monitoring, they need (2) to be able to apply EEG monitoring correctly. To enable users to interpret EEG monitoring for guiding anaesthetic level, they have (3) to understand how EEG monitoring could indicate (3a) too shallow, (3b) adequate or (3c) too deep anaesthesia. To be able to be sure that recognised signs of too shallow, adequate or too deep anaesthesia are actually valid, they need (4) to be able to identify artefacts, which requires (5) to understand how EEG monitoring works (physiologically and technologically) and (6) to understand the different types of information visualisation on EEG monitors (raw EEG, spectrogram, processed indices). Moreover, as different anaesthetics manifest with distinct effects on the EEG, it is necessary for users (7) to know about the different EEG patterns induced by different substances used for anaesthesia. To avoid confusing patterns caused by nociception and insufficient dosing of analgesics with patterns of a too shallow hypnotic depth, they require (8) to be able to identify signs of nociception in the EEG. And finally, to adapt the knowledge to specific patient populations, they are required (9) to know about EEG differences in geriatric as well as in paediatric patient populations.
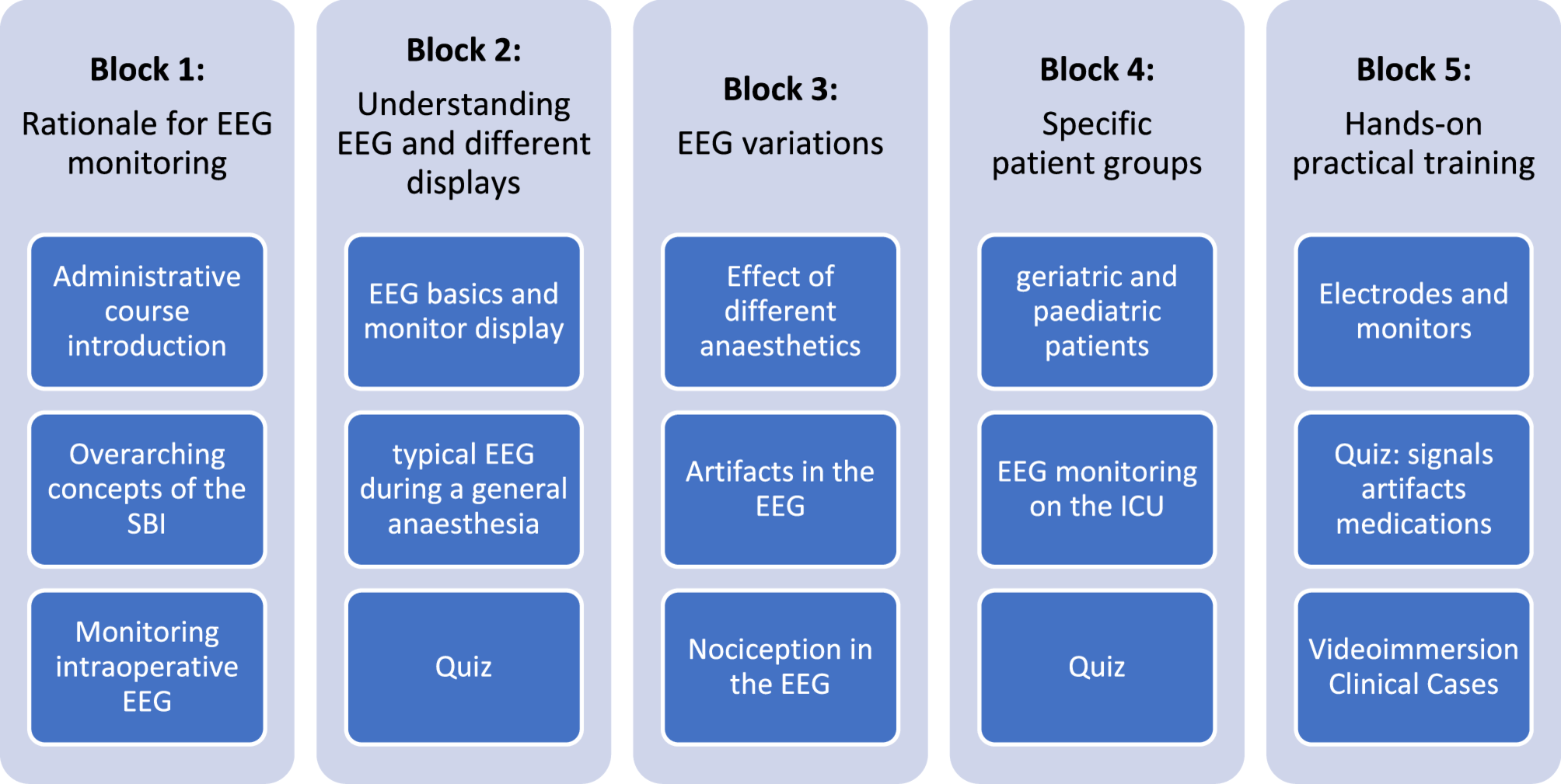
Structure of the SBI’s EEG boot camp for anaesthesiaAs the order in which we logically derived the learning goals is not necessarily the best order in which to teach their contents, we restructured the course contents into four theoretical blocks that build on each other, concluding with a final block providing consolidation for training (see Fig. 1).
Fig. 1 Block 1: Rationale for EEG monitoring during anaesthesia
Block 1: Rationale for EEG monitoring during anaesthesiaAfter an administrative introduction into the course, the second part of the first block aims at putting EEG monitoring in the context of the general approach of an outcome-focused anaesthesia practice, which is the overarching concept of the Safe Brain Initiative. After this general motivation to enhance patient outcomes by optimizing patient care, the course narrows its focus to EEG monitoring. It presents specific evidence on how too deep or too shallow anaesthesia can impact outcomes and illustrates how EEG monitoring can aid in avoiding these scenarios. A key focus is on burst suppression, an EEG pattern marked by low-amplitude periods interrupted by bursts of activity. Burst suppression is recognised as a potential risk factor for the development of postoperative neurocognitive disorders [24, 25]. However, some contradictory findings [26] led to the European Society of Anaesthesiology’s ‘weak’ recommendation for EEG-based monitoring [20]. Due to the non-standardized and unreliable automated detection of burst suppression in monitoring systems [17, 19], it is crucial to include raw EEG and DSA analysis, which is a primary motivation for this course.
Block 2: Understanding the EEG and the different displays of the monitor What does the EEG measure and how does the monitor display information?The second block starts with one lecture providing fundamental knowledge on how the EEG is measured from a physiological, technical and practical perspective. Beginning with the physiological introduction, knowledge is provided on what the EEG actually is, including a short description of how the EEG and its synchronous activity are generated by the (cortical) neurons and how the raw EEG is abstracted into DSA and index values. After the basics of EEG physiology, in the technical introduction, we demonstrate how the raw EEG, the DSA and the indices are presented on the monitoring systems and how the display can be optimised for clinical decision-making. Concluding with the practical introduction, we teach the basics of how to properly set up anaesthesiologic EEG monitoring, including different possibilities of recording setups and covering the complete process from identifying the site for monitoring, skin preparation, proper electrode attachment, and how to maintain a good recording quality throughout a case.
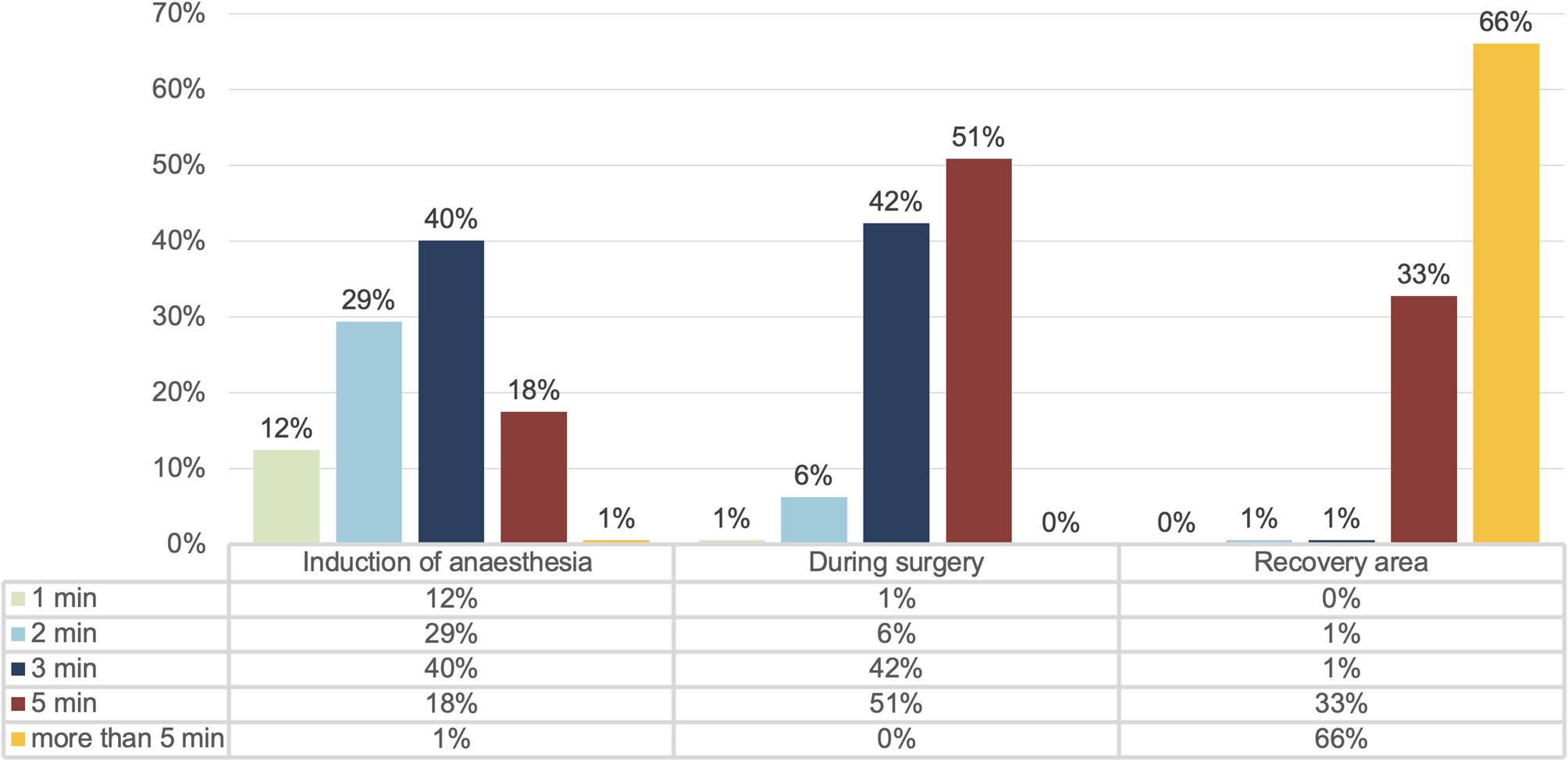
What does EEG monitoring show during a typical general anaesthesia?After laying the groundwork for EEG monitoring in the first lecture, the second lecture actively builds upon this knowledge by presenting the first exemplary cases. This session focuses on relatively straightforward general anaesthesia cases without complicating factors, highlighting typical EEG patterns during induction, maintenance, and recovery from anaesthesia. Additionally, it provides practical algorithms on how EEG monitoring can guide or assist at each stage.
Quiz to activate and repeat knowledge of blocks 1 + 2The second block concludes with a dynamic online quiz to activate participants'knowledge. Participants answer multiple-choice questions from lectures in blocks 1 and 2 through their smartphones, using platforms (e.g. using kahoot.com). Following their submissions, the system displays the answer distribution, and the respective lecture speaker explains the correct answers. Although we present test results anonymously, participants can use nicknames for personalised feedback.
This quiz engages participants in decision-making, thereby triggers them to activate knowledge gained up to this point and reinforces crucial points through the speakers'explanations. It transitions the format from lecture-based to interactive, inviting participants to ask questions about topics from the first two blocks. This setup encourages discussions, which participants can extend into the following break for more personalised interactions.
Block 3: Identifying EEG variations depending on the situation How do I recognise the effect of different anaesthetics in the EEG?Since the second block has provided the basics of EEG monitoring and what to expect in a typical patient during the different phases of general anaesthesia, the third block focuses on introducing variability. The first and most important aspect of variability in EEG monitoring during general anaesthesia is the heterogeneity of EEG patterns induced by different anaesthetics. Thus, this lecture describes how typical GABAergic anaesthetics and non-GABAergic substances influence the intraoperative EEG differently and how the processed EEG indices react to these changes.
It’s highlighted that processed EEG indices, originally designed to reflect the anaesthetic level induced by GABAergic substances (notably the slowing of the EEG and the emergence of delta rhythms [27]), may lose their validity with other substances like ketamine or dexmedetomidine that produce different EEG patterns. Particularly, ketamine can cause oscillatory activity in higher frequencies (around 30 Hz), potentially increasing index values despite a deeper anaesthetic level [28], depending on the ketamine concentration [29].
Importantly, regardless of the EEG indices, all these substances create unique signatures in both the EEG and the DSA. Thus, this module educates participants on how visual analysis of the EEG, augmented by DSA, can effectively identify the effects of various anaesthetics and aid in guiding anaesthesia. This is especially relevant when processed indices may not be reliable due to the use of non-GABAergic drugs.
How do I recognise artefacts in the EEG?The perioperative period, being susceptible to various disturbances, often results in physiological and technical EEG artefacts, adding further variability to measurements. Addressing this, the second lecture in this block concentrates on the most common artefacts, offering algorithms to identify them and pinpoint their sources. This lecture also explains how artefacts can result in scenarios where no index is displayed due to a contaminated EEG signal. Moreover, it details how such contaminated signals can mislead the processed EEG indices, causing them to display inaccurately high or low values [30,31,32].
How do I recognise nociception in the EEG?Contrary to common perception, the'depth'or level of general anaesthesia is not a unidimensional phenomenon [33]. Particularly when anaesthesia involves a combination of anaesthetics and potent anti-nociceptive substances like opioids, it’s crucial to consider the nociception vs anti-nociception balance as a separate yet interconnected dimension from the hypnosis vs arousal balance [34]. Nociception and anti-nociception, primarily mediated by spinal-subcortical processes, cannot be directly monitored by cerebrocortical EEG, which focuses on the hypnotic component of anaesthesia. However, nociception, acting as a potent arousing stimulus, can be indirectly reflected in EEG changes such as an alpha dropout [35, 36], a delta arousal [37, 38] or a beta activation [5, 39, 40].
This lecture introduces participants to the multidimensional nature of anaesthesia. It covers how nociceptive processing continues during general anaesthesia, its impact on patient outcomes, and how nociception can be spotted in the raw EEG, the DSA, and the processed EEG indices. The lecture also provides clinical algorithms to distinguish responses from those due to nociception from those due to non-nociceptive arousal.
Block 4: Identifying EEG variations depending on patient characteristics What is different in geriatric and paediatric patient populations?The fourth block delves into additional factors that introduce variability in EEG monitoring, emphasising that substances and a patient's age can affect the EEG under anaesthesia, thereby influencing processed EEG data [41,42,43]. In this block's first lecture, age-specific changes observable in the EEG monitoring of geriatric and paediatric patients are discussed. While the primary focus of this boot camp is on adult patients, there's a brief exploration of EEG differences in infants before shifting to age-induced EEG changes in adults. The lecture highlights that most monitoring systems do not account for age in index calculation. Therefore, it guides on how to interpret the index, raw EEG, and DSA, particularly in the geriatric population and patients with a frail brain [44, 45].
How can I transfer my expertise from the operating room to sedation in the ICU?To synthesise and apply the knowledge acquired so far, this discussion block presents exemplary ICU cases. These cases are designed to explore the potential application of anaesthesiologic EEG monitoring to manage ICU patients'sedation levels. This shift from the operating room to the ICU context and from general anaesthesia to ICU sedation challenges participants to abstract and transfer their knowledge, aiding consolidation.
Quiz to activate and repeat knowledge of blocks 3 + 4The fourth block includes a second interactive online quiz for knowledge activation, similar to the first. Multiple-choice questions from the lectures in blocks 3 and 4 are presented, and participants submit their answers through their smartphones. The respective speakers then explain the correct answers, mirroring the approach of the first quiz.
Block 5: Repetition for consolidation and practical trainingThe last teaching block of the course provides further repetition of the content, but in a practical hands-on setting. To reduce the size of the complete group of participants for practical hands-on training, it is split into three sub-groups, which rotate through three different stations:
Split-group Station 1: Placing the electrodes and operating the monitorsThis hands-on station is dedicated to teaching practical skills in setting up and operating EEG monitors. The lecturers first demonstrate various recording setups, encompassing the entire process from selecting the monitoring site, preparing the skin appropriately, and attaching the electrodes properly. This includes showcasing alternative setups like mandibular or nasal montages. Participants are also guided through the different monitor settings, such as filter, time, and amplitude adjustments, and how to access various types of information like impedance, signal quality, raw EEG, DSA, and indices. After the demonstration, participants can practice with monitors (ideally from all available brands) on each other, allowing them to experiment with the different equipment.
Split-group Station 2: Quiz about signals, artefacts and medication signaturesThe second station offers a playful quiz integrating different aspects of EEG monitoring, focusing on distinguishing between various signals, artefacts, and anaesthetic substance signatures. This interactive activity consolidates learning from the theoretical blocks by challenging participants to apply their knowledge fun and engagingly.
Split-group Station 3: Video immersion into clinical casesIn this station, the focus shifts to understanding the role of EEG monitoring within the broader clinical context of general anaesthesia. Participants watch complete anaesthesia cases, from pre-anaesthesia preparation to post-anaesthesia care, captured through multiple cameras. These videos showcase the complexity of clinical situations, highlighting how to incorporate EEG monitoring into specific clinical processes without detracting from other vital procedures and monitors. This immersive experience helps participants to appreciate the practical application of EEG monitoring in a real-world setting.
Block 6: DebriefingThe course concludes with a debriefing block, mirroring the administrative introduction at its start. This final segment aims to address any remaining questions, gather oral feedback, and collect written evaluations from the participants. Additionally, participants are guided on how to continue expanding their knowledge post-course, including directions on where to find further information and seek guidance for specific queries.
All participants will be granted access to a dedicated website, enabling them to share specific questions and interesting cases with their peers and course instructors. Similar to the course introduction, special attention is given to allotting sufficient time for this debriefing. This ensures that participants leave the course feeling well-informed and oriented, significantly influencing their overall attitude towards the course, its content, and learning outcomes. Consequently, the duration of the debriefing is planned to be equal to that of the split-group stations in the previous block, ensuring a comprehensive and satisfying course conclusion.
Investigation of the effects of the courseTo assess the effect of the SBI’s EEG boot camp for anaesthesia on the participants’ knowledge of the defined learning goals and their attitudes toward incorporating EEG monitoring into routine anaesthesia practice, we compared participants’ self-ratings on Likert scales (0–5) before and after the course (questionnaire shown in supplement 2). For this purpose, we obtained anonymous ratings of the participants before and after the 2023 course, held in Greifswald, Germany. As participation in the evaluation was voluntary for the participants and fully anonymous, the need for a formal ethics approval and written informed consent was waived by the local ethics committee (Ethikkommission– Universitätsmedizin Greifswald).
A formal power analysis was not performed due to the exploratory nature of the investigation regarding the size of the effects of the course. Pre- and post-course ratings were compared using the paired Wilcoxon signed-rank test, with a significance threshold set at p < 0.05.
Comments (0)