Search strategy
This systematic review and meta-analysis were performed and reported in accordance with the Cochrane Collaboration Handbook for Systematic Review of interventions and the Preferred reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [9] Statement guidelines.
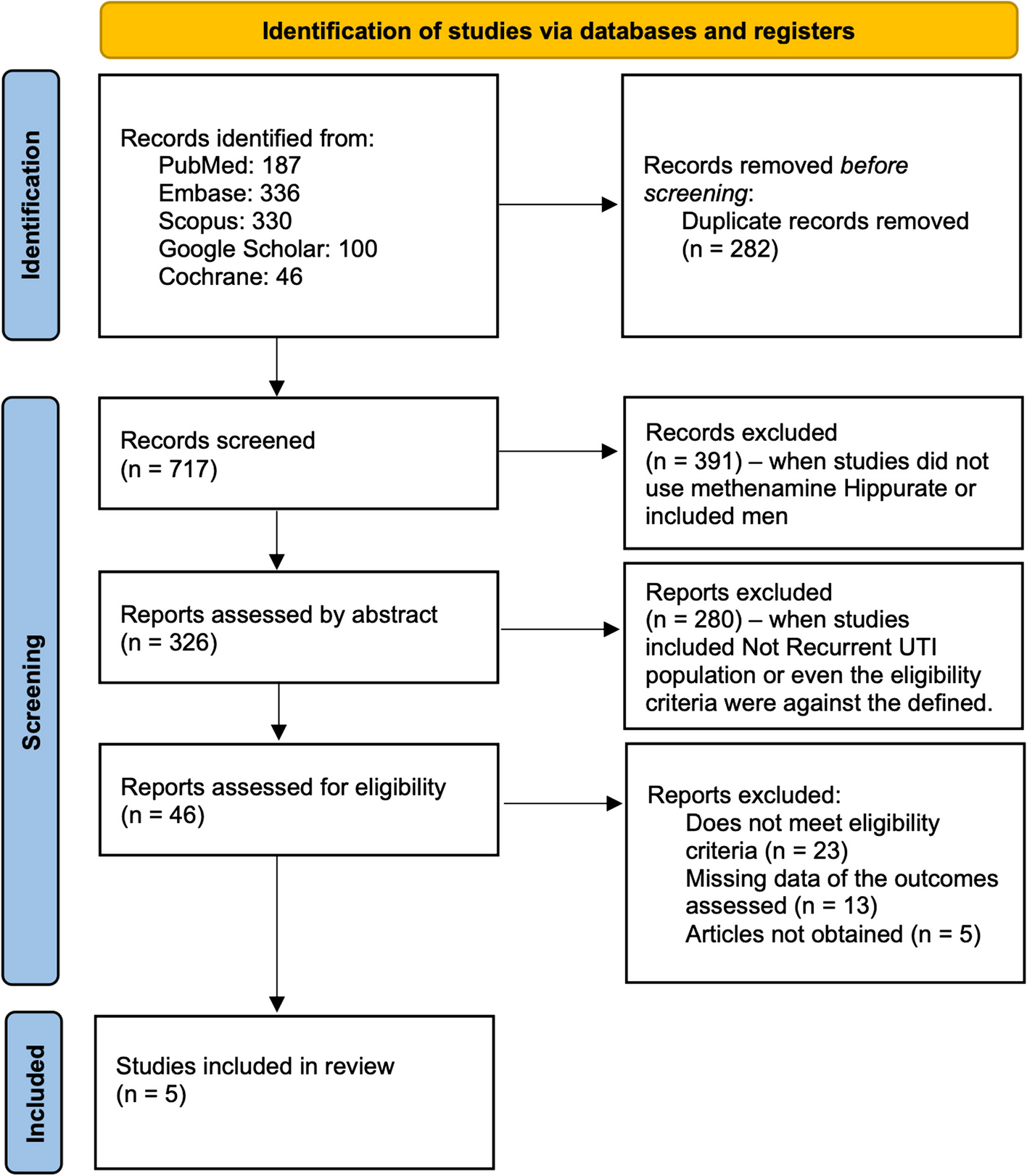
We conducted a comprehensive search of MEDLINE, Embase, Scopus, and Cochrane CENTRAL, along with Google Scholar for additional internet sources, from their inception until March 2024 for randomized controlled trials of methenamine hippurate vs antibiotic/placebo trials in women with recurrent urinary tract infection. Please refer to appendix our search strategy. A highly sensitive search strategy was also used in a way to better identify randomized trials in the databases.
The references from all included studies, previous systematic reviews and meta-analyses were also searched manually for any additional studies. The prospective meta-analysis protocol was registered on PROSPERO under protocol CRD42024512556.
Eligibility criteria for study selection
We included randomized controlled trials (RCTs) that assessed adult women (aged ≥ 18 years) with a history of recurrent or confirmed UTIs. Studies were eligible if they compared the efficacy of methenamine hippurate with placebo/no treatment or any antibiotic and reported at least one of the clinical outcomes of interest. We excluded non-randomized controlled trials (non-RCTs), studies without a methenamine arm or without a comparison to placebo/antibiotics, studies involving women with catheters, patients with anatomical abnormalities (e.g., solitary kidney, ureteral or urethral stricture), or patients with active urinary tract infections.
The exclusion of women with active UTIs was critical for the integrity of this review since our purpose with this work is to evaluate methenamine hippurate as prophylaxis method for recurrent UTIs, not for the treatment of active infections. Including women with active UTIs could introduce significant confounding, as the focus of this review is on the prevention of future UTI episodes, rather than the treatment of an ongoing infection. By excluding women with active UTIs, we ensured that the results reflect the true prophylactic effect of methenamine hippurate. We also excluded studies that reported the use of acidifying agents in combination with methenamine hippurate, as these could interfere with the outcomes of interest. Case reports, systematic reviews, and bibliographic reviews were excluded to maintain a high standard of evidence.
Outcomes
The primary outcome was the recurrence of clinical UTIs, as defined by the presence of any of the following symptoms: dysuria, nocturia, urgency, fever, urinary frequency, burning, suprapubic pain, and loin pain. This outcome was chosen because recurrent UTIs are most commonly diagnosed based on clinical symptoms in women, with symptoms being the primary guide for treatment decisions. While microbiological confirmation (e.g., positive urine culture) would provide a more objective measure of UTI, clinical symptoms alone are frequently sufficient for diagnosing recurrent UTIs in clinical practice. The secondary outcomes included positive urine cultures associated with UTI symptoms, asymptomatic bacteriuria, and adverse effects (e.g., nausea, diarrhea, rash, and others).
Screening
After deduplication, in which we used Endnote online™ 20 (Clarivate, Philadelphia, PA) [10], two independent researchers (NH and GO) screened the studies by title and abstract, and disagreements were solved by a third (JC). Following this process, full text screening was performed. No automation tools were used during the screening process.
Data extraction and quality assessment
Two authors (BP and NH) independently extracted the data based on a predefined protocol and disagreements were solved by a third (JC). The data primarily assessed were the type o study, the language of each paper, number of patients enrolled, mean age of patients, methenamine dosage, which antibiotic was used and each dose, the duration of follow-up, and all the outcomes previously mentioned. Risk of bias was assessed in randomized studies using version 2 of the Cochrane Risk of Bias assessment tool (RoB 2) [11]. Two independent authors completed the risk of bias assessment (NH and GO). Disagreements were resolved through a consensus after discussing reasons for discrepancy. Regarding the UTI definition of each study included, it was not possible to obtain since it was lacking in the majority of them.
Statistical analysis
Dichotomous data are presented as relative risk (RR) with 95% CI. Pooled estimates were calculated with the random-effects model, considering that the patients came from different populations. We considered a study to exhibit considerable heterogeneity if, following the statistical analysis, the I2 statistic is equal to or greater than 30%.
We performed a Trial Sequential Analysis (TSA) (alpha = 5%, beta = 90% for a relative risk reduction of 5%) focusing on type 2 errors for the main outcome. It may be useful to explain that Trial Sequential Analysis (TSA) is a valuable tool in meta-analyses as it helps control random errors, particularly when data is sparse or when repeated significance testing occurs. By applying monitoring boundaries, TSA assesses whether a meta-analysis has sufficient information to draw reliable conclusions or if additional studies are necessary. It also helps avoid type I (false positive) and type II (false negative) errors. In the context of my meta-analysis, TSA is valuable because it allows us to determine whether the available evidence is robust or if further trials are needed, ensuring the reliability of our conclusions RStudio Team (2020). RStudio: Integrated Development for R. RStudio, PBC, Boston, MA URL, was the software used for statistical analysis [12].




Comments (0)