
Remember me



The median follow-up time was 51 months (range: 12–110 months). By the end of the follow-up period, 101 (90.2%) patients had completed follow-up, and 11 (9.8%) were lost to follow-up. A total of 112 patients with pT1 ~ 4N1M0 stage RCC were included in this study. Among them, 74 were male and 38 were female, with a mean age of (49 ± 14) years. All patients underwent radical nephrectomy combined with regional lymph node dissection. The median maximum tumor diameter was 7.6 (5.4, 10.1) cm. Postoperative pathological T stages were as follows: pT1 in 22 patients, pT2 in 10 patients, pT3 in 67 patients, and pT4 in 13 patients. Preoperative lymph node enlargement was observed in 67 patients. The median number of lymph nodes dissected during surgery was 8.0 (4.0, 13.0), and the median number of lymph node metastases in postoperative pathology was 2.0 (1.0, 6.0). The median number of lymph node metastases in patients with pT2 or lower was 2.0 (1.0, 4.0), while in patients with pT3 or higher, it was 3.0 (1.0, 6.8). Pathological types included clear cell carcinoma in 43 cases (38.4%), papillary carcinoma in 26 cases (23.2%), chromophobe cell carcinoma in 4 cases (3.6%), and other types in 39 cases (34.8%). The intraoperative complication rate was 3.6% (4/112), including 4 cases of hemorrhage (transfusion volume 250 ml). The postoperative complication rate was 5.4% (6/112), with 5 (4.5%) Grade II and 1 (0.9%) Grade III complications (Clavien-Dindo classification). Postoperative complications included incisional infection (2 cases, Clavien II), atelectasis (2 cases, Clavien II), other minor complication (1 case, Clavien II), and urinary tract infection (1 case, Clavien III) (Table 1).
Table 1 Basic information of 112 patientsThe 5-year overall survival (OS) rate was calculated using the Kaplan-Meier method. By the end of follow-up, 11 patients were lost to follow-up and were treated as censored data. The 5-year OS rate was 17.2% (95% CI: 10.5%−24.9%). Postoperatively, a total of 58 patients exhibited tumor progression. This included 9 cases of local recurrence, with 8 of these cases recurring in regional lymph nodes and 1 in the ipsilateral adrenal gland. Additionally, 54 patients developed distant metastasis, comprising 25 with extraregional lymph node metastasis, 17 with lung metastasis, 18 with bone metastasis, and 7 with liver metastasis. Throughout the follow-up period, 59 patients ultimately succumbed to their disease. Of the 58 patients who experienced tumor progression, 21 received systemic therapy: 14 (66.7% of those treated) received PD-1 inhibitor immunotherapy, 6 (28.6%) received tyrosine kinase inhibitor (TKI) targeted therapy, and 1 (4.7%) received supportive care only as their primary post-progression treatment. Among the 54 patients who did not experience tumor progression, 4 (7.4%) received adjuvant therapy, whereas among the 58 patients who did progress, 17 (29.3%) received adjuvant therapy, typically initiated after progression was detected. A direct comparison of recurrence risk based on postoperative adjuvant therapy was challenging due to this selection bias. However, in an exploratory analysis of high-risk patients (pT3/4), those who received adjuvant therapy (n = 6) showed a trend towards longer RFS compared to a matched group who did not (n = 12), although this was not statistically significant (median RFS 15.2 vs. 9.8 months, p = 0.18), highlighting the need for larger, prospective trials.
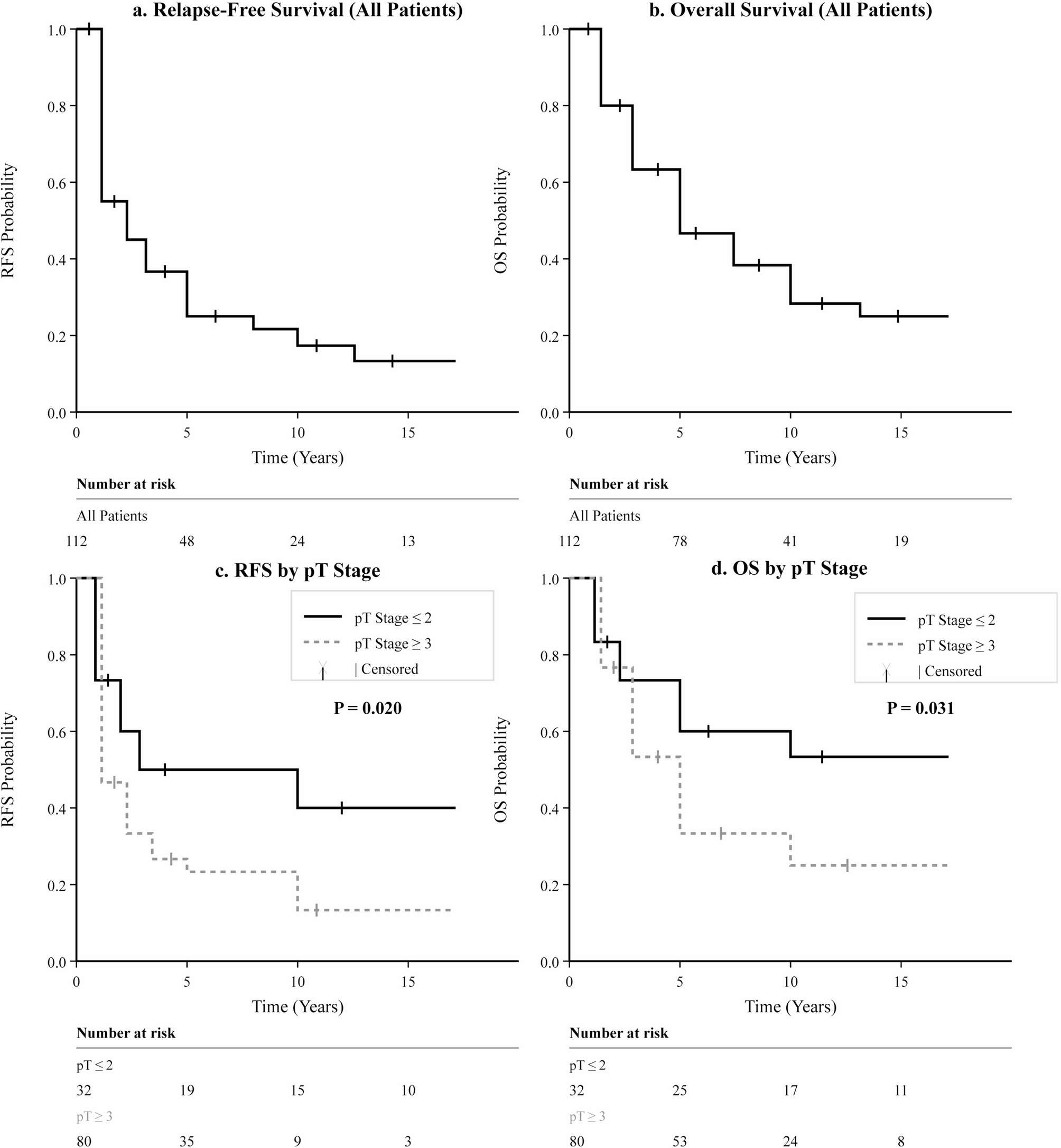
The median relapse-free survival (RFS) after surgery was 0.90 (0.35, 2.60) years, with 1-, 3-, and 5-year RFS rates of 44.6%, 21.5%, and 12.1%, respectively. The median overall survival (OS) was 2.25 (1.15, 4.10) years, with 1-, 3-, and 5-year OS rates of 78.5%, 36.8%, and 17.2%, respectively (Fig. 1).
Fig. 1
Kaplan-meier survival curve analysis and pT stage-stratified survival curves for OS of 112 patients (a) RFS Curve; (b) OS curve; (c) pT Stage-Stratified RFS curve; (d) pT Stage-Stratified OS curve
Multivariate Cox proportional hazards regression analysis of patient survival/death outcomes revealed that postoperative tumor progression and sarcomatoid differentiation in pathology were independent risk factors for poor overall survival (P = 0.001 and P = 0.001, respectively; Hazard Ratios (HR) and 95% Confidence Intervals (CI) are detailed in Table 2). Kaplan-Meier survival curve analysis demonstrated that patients with postoperative tumor progression and sarcomatoid differentiation experienced significantly worse survival outcomes (P < 0.05), as summarized in Table 2; Fig. 2.
Table 2 Univariate and multivariate Cox regression of overall survival time after surgeryFig. 2
Kaplan-meier survival curve analysis of postoperative survival prognosis in 112 patients (a) OS curve for Sarcomatoid Differentiation Group; (b) OS curve for tumor progression group
Subgroup analyses revealed that patients with pN1 (1–2 positive nodes) had a significantly higher 5-year RFS rate (52%) after LND compared to those with pN2-3 (≥ 3 positive nodes) (20%, P = 0.010). The local recurrence rate was lower in patients with clear cell RCC (5.8%) than in those with non-clear cell RCC (11.6%, P = 0.039).
Risk factors for tumor progressionA total of 58 patients experienced tumor progression (recurrence and metastasis) postoperatively, of which 43 (74.1%) died due to tumor progression. Multivariate Cox proportional hazards regression analysis showed that patients with preoperative lymph node enlargement had a significantly higher risk of tumor progression (P = 0.021; HR and 95% CI detailed in Table 3). Furthermore, multigroup regional lymph node metastasis was associated with tumor progression in univariate analysis but did not maintain significance in multivariate analysis (detailed in Table 3). Kaplan-Meier survival curve analysis demonstrated that patients with preoperative lymph node enlargement had worse RFS (P < 0.0001) (Table 3; Fig. 3).
Table 3 Univariate and multivariate Cox regression of postoperative tumor progressionFig. 3
Relapse-free survival curve in patients with preoperative lymph node enlargement (a) RFS curve; (b) OS curve
Subgroup analysis - risk factors for distant metastasisAmong the 54 patients who developed distant metastasis postoperatively, multivariate Cox proportional hazards regression analysis revealed that those with preoperative lymph node enlargement were significantly more likely to experience distant metastasis following surgery. This finding indicates that preoperative lymph node enlargement serves as an independent risk factor for distant metastasis (P = 0.038; HR and 95% CI detailed in Table 4). Furthermore, Kaplan-Meier survival curve analysis demonstrated that patients with preoperative lymph node enlargement exhibited significantly worse RFS and OS (P < 0.05). These findings are detailed in Table 4 and illustrated in Figs. 3 and 4.
Table 4 Univariate and multivariate Cox regression analysis of distant metastasis after surgeryFig. 4
Overall survival curve in patients with preoperative lymph node enlargement (a) RFS curve; (b) OS curve
Subgroup analysis - factors influencing local tumor recurrenceNine patients experienced local recurrence postoperatively. Among them, 6 patients had a pT stage of ≥ pT3a, and the pathological types were papillary RCC (7 cases), poorly differentiated RCC (1 case), and renal collecting duct carcinoma (1 case). Six patients died, with pathological diagnoses of papillary RCC (5 cases) and poorly differentiated RCC (1 case). Univariate Cox proportional hazards regression analysis indicated that maximum tumor diameter, pT stage, preoperative lymph node enlargement, number of lymph node metastases, intraluminal tumor thrombus, tumor necrosis, and sarcomatoid differentiation had no significant impact on local recurrence (P > 0.05). Multivariate Cox proportional hazards regression analysis indicated that patients with multigroup regional lymph node metastasis exhibited a significantly higher likelihood of experiencing local recurrence postoperatively (P = 0.031; HR and 95% CI detailed in Table 5). This suggests that multigroup regional lymph node metastasis constitute an independent risk factor for local recurrence. Additionally, Kaplan-Meier survival curve analysis revealed that patients with multigroup regional lymph node metastasis had notably worse postoperative RFS and OS (P < 0.05). Detailed results are presented in Table 5 and illustrated in Fig. 5.
Table 5 Univariate and multivariate Cox regression analysis of local tumor recurrence after surgeryFig. 5
Survival curve analysis in patients with multigroup regional lymph node metastasis (a) RFS curve; (b) OS curve
Comments (0)