Our study, the largest cohort of necrozoospermia patients described to date, demonstrates that the presence of a post-testicular cause, especially a seminal tract anomaly is a risk factor for severe necrozoospermia. Other causes separately or combined do not seem to worsened it.
Correlation analyses between age and necrozoospermia showed a negative, but statistically weak effect. This observation has already been reported in the literature, particularly at the age of 35 and above [19, 20]. The link between sperm necrosis and aging is in line with the increase of reactive oxygen species (ROS) and DNA fragmentation in advanced paternal and a dysregulation in the secretion of seminal plasma enzymes that regulate sperm death [19, 21]. It is known that reactive oxygen species produced by mitochondria affect the integrity of the sperm genome and epigenome. This, in turn, influences the processes of spermatogenesis and spermiogenesis [22].
The FSH level was inversely correlated with sperm necrosis. It should be analyzed with testicular volume, which was significantly higher when necrozoospermia was severe. The comparison of inhibin B levels between the severity groups did not reveal any significant difference. FSH acts through its receptors on Sertoli cells in spermatogenesis. It allows Sertoli cells to stimulate spermatogonia production and maturation. Along with intratesticular testosterone, FSH has an anti-apoptotic effect on germ cells [23]. This may explain why necrozoospermia remains moderate or even mild despite high FSH levels in some patients. Inhibin B, FSH and testicular volume are markers of Sertoli cells function and spermatogenesis. In this study, patients with severe necrozoospermia had a normal FSH level and testicular volume. Furthermore, there was no significant difference in sperm concentration between the severity groups, but seminal volumes were significantly lower in the severe necrozoospermia group compared to the other ones. This suggests functioning Sertoli cells, whereas a post-testicular cause explains the decreased sperm vitality. In this work, post-testicular anomaly was mainly from epididymal origin. Epididymis is responsible for about 5% of the seminal plasma secretion, this explains why the ejaculate volume was within the WHO norms (> 1.4mL) in the severe necrozoospermia group and why there was no significant difference for the seminal pH analysis between the groups.
In the literature, obesity is associated with a significant decrease in sperm vitality [24, 25]. Obesity induces a chronic inflammatory process in the seminiferous tubules and epididymis through an increased production of ROS and inflammatory mediators. As a result, it alters the systemic and local environment necessary for spermatogenesis and sperm maturation in the epididymis [24]. Also, increased scrotal temperatures due to abdominal and scrotal adiposity may impair sperm vitality [26]. However, in this study, no significant relationship was found between the BMI and necrozoospermia. The prospective study by Eisenberg et al. [27] compared sperm parameters according to BMI in a cohort of over five hundred men. There was no impact of BMI value on sperm vitality or on the DNA fragmentation index for the patients suffering from necrozoospermia.
In this study, no correlation was found between the severity of necrozoospermia and active smoking. A prospective study of 95 patients divided into two groups (smokers and non-smokers) by Mostafa et al. [28] showed a significant impact of smoking on sperm concentration, motility and vitality. Smoking increases ROS production which consequently induces a significant decrease in the seminal plasma antioxidant properties [28]. Moreover, this oxidative stress would significantly increase DNA fragmentation and chromatin condensation anomalies in the sperm nucleus [26]. Regarding the impact of cannabis, few patients reported active and regular cannabis use in this series. No analysis could therefore be performed despite the known negative effect of cannabis on sperm vitality [8].
Copens et al. [13] investigated the impact of seminal tract anomalies on fertility and lower urinary tract symptoms. In this prospective study, 65 prostatic utricles were diagnosed by transrectal ultrasound complicated or not by an ejaculatory duct anomaly or a uni or bilateral dilatation seminal vesicles. 12% of the men suffered from infertility, among them 25% presented with necrozoospermia. Seminal tract abnormalities can be involved in male infertility when associated with other signs of obstruction such as hypospermia, abnormal seminal plasma secretion, severe oligospermia or azoospermia [13]. Seminal plasma allows sperm to be transported through the excretory tract under stable conditions (physical, biochemical and bacteriological). Any change in its composition can alter the spermatozoa vitality [29]. Epididymal cysts frequently observed during sonographic assessment are not associated with infertility [30].
Seminal tract anomalies may be the consequence of a genital infection such as epididymitis or prostatitis. The epididymal transit allows the spermatozoa to acquire its motility and fertility functions. However, in the case of repeated epididymitis, the epididymal epithelium can be altered which explains the alteration in sperm parameters [12]. Acute, sub-acute or chronic bacterial infections can also have a negative impact on male fertility. In most situations of male hypofertility, the major pathogens found are: Escherichia coli, chlamydia trachomatis, ureaplasma urealyticum, mycoplasma hominis and mycoplasma genitalium [10, 31]. These bacteria will cause an inflammatory response in the seminal tract. The recruitment of leukocytes and the excessive secretion of inflammatory mediators such as certain cytokines and/or ROS which will then disrupt spermatogenesis, post-testicular sperm maturation processes, modify the degree of sperm chromatin condensation and finally increase the rate of sperm DNA fragmentation [32, 33]. Furthermore, in the event of a breach in the blood-testis/genital tract barrier due to a substantial infectious or inflammatory process, the formation of anti-sperm antibodies (ASA) may occur [34].
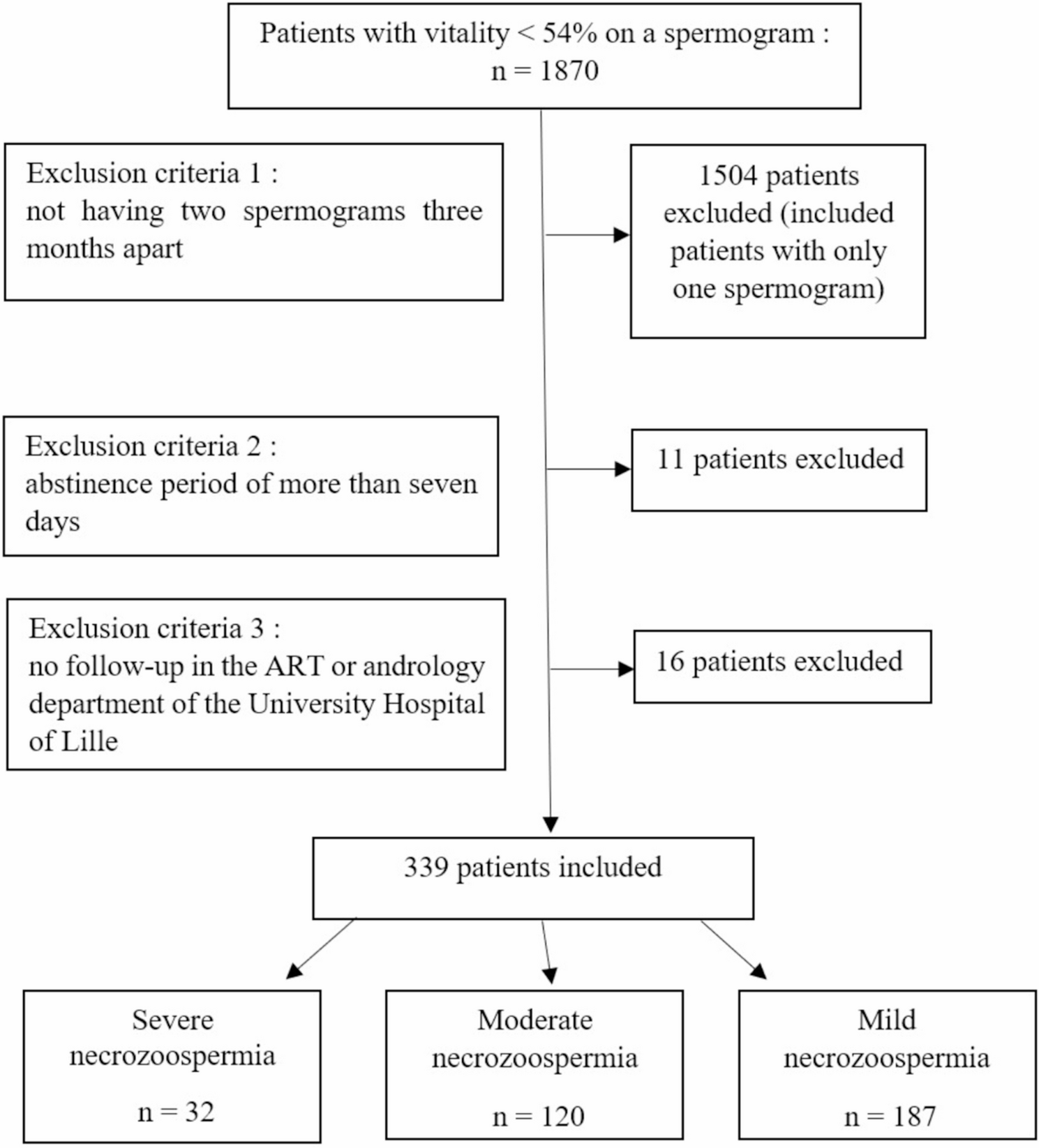
Few studies have investigated the impact of etiology on the severity of necrozoospermia. The review of the literature by Boursier et al. [3] found that patients with a post-testicular anomaly had more severe necrozoospermia compared to patients with mixed etiologies. In this study, the presence of a seminal tract anomaly would significantly increase necrozoospermia. Further analysis did not show an additive or synergistic effect of the accumulation of risk factors and/or pathologies on the severity of necrozoospermia. Depending on the severity group, between 26 and 28% of the patients had several etiologies of necrozoospermia. The presence of a post-testicular anomaly was identified as the sole risk factor associated with the severity of necrozoospermia. Consequently, if a patient exhibited an additional risk factor of mixed or testicular origin, the impact on the deterioration of sperm vitality might be minimal.
The epididymis could constitute a hostile environment, where spermatozoa would be exposed to oxidative stress [4, 35]. Wilton et al. [35] studied the composition of seminal plasma and the ultrastructure of testicular and ejaculated sperm in four men with asthenozoospermia (0–16% total motility) and necrozoospermia (2–45% vitality). This retrospective study demonstrated that the seminal plasma composition and the testicular spermatozoa ultrastructure were found to be within normal limits. This finding stands in contrast to the ultrastructure of ejaculated spermatozoa, which was found to be abnormal. This finding indicates that sperm death may occur during transit or storage in the epididymis. This hypothesis is corroborated by the improvement in sperm parameters after repeated ejaculations [35]. According to these articles, when no etiology is found, it is considered to be epididymal necrozoospermia. However, it is important to notice that these studies were carried out on small samples. It would seem more appropriate to separate necrozoospermia of idiopathic origin from post-testicular origin due to seminal tract anomalies documented by ultrasound. In our study, 21% had an idiopathic cause of necrozoospermia, which is in agreement with the data published in the literature [6].
None of the patients with a history of inguinoscrotal surgery had agglutination on semen analysis. Consequently, it was not possible to classify them as ‘autoimmune’ necrozoospermia. The link between ASA and sperm necrosis is controversial. Cui et al. meta-analysis [16] of 8 studies with 238 cases of infertile patients with ASA and 929 cases without ASA found a negative impact of ASA on sperm concentration and motility but no impact on sperm morphology and vitality. A recent review of the literature highlights that ASA is linked to a drop in sperm motility, vitality, and sperm count [36]. The presence of ASA should be suspected and tested in cases of pelvic surgery history, testicular trauma or testicular torsion or sperm agglutination regardless of whether they are associated with alterations in sperm parameters [37].
Various limitations of the study warrant mention. Data of this retrospective work are missing, mainly in the mild necrozoospermia group. In the event of sperm vitality between 40 and 54%, patients did not always have a complete andrological check-up, consisting of clinical examination, testicular ultrasound and hormonal assays if the other sperm parameters were normal, which might participate to the lack of significance for the analysis.
However, this is the largest group of patients with necrozoospermia studied so far. All hormonal assessments were analyzed in the hormonology laboratory of the Lille University Hospital, and all ultrasounds were performed by an experienced radiologist in the genitourinary imaging department of the same hospital.
In our study, none of the patients included had a spinal cord injury. This is directly related to the exclusion criteria of sexual abstinence for more than seven days. At Lille University Hospital, there’s a special process for these patients. They have a special place where sperm is collected and then studied at the CECOS (Centre d’Etude et de Conservation des Œufs et du Sperme – Center for sperm conservation and study). At the CECOS, sperm vitality is not studied on the fresh ejaculate before freezing (only concentration and motility are analyzed).




Comments (0)