
Remember me



A total of 10 patients with T1 stage renal tumors, enrolled between March and July 2023, were prospectively included in this study. The inclusion criteria included the following: (i) patients with renal tumor and clinical stage were limited to T1NoMo, which was confirmed by image examination; (ii) patients aged 16–85 years. The exclusion criteria included the following: (i) patients with renal tumors near renal hilus or invading the renal sinus area that may require simultaneous occlusion of the renal vein during the resection of the tumor; (ii) patients whose tumor is supplied by multiple arteries and is difficult to block with one balloon; and (iii) patients with severe cardiovascular and cerebrovascular diseases, especially with large vascular lesions. Informed consent was obtained from all patients, and assessments were conducted by the same physician. A preoperative evaluation was jointly performed by one surgeon and one specialized sonographer, based primarily on preoperative ultrasound, contrast enhanced CT, and CTA (only for cases requiring branch artery occlusion).
This study was registered in the Chinese Clinical Trial Registry and approved by the institutional ethics review board. This work has been reported in line with the STROCSS criteria [12].
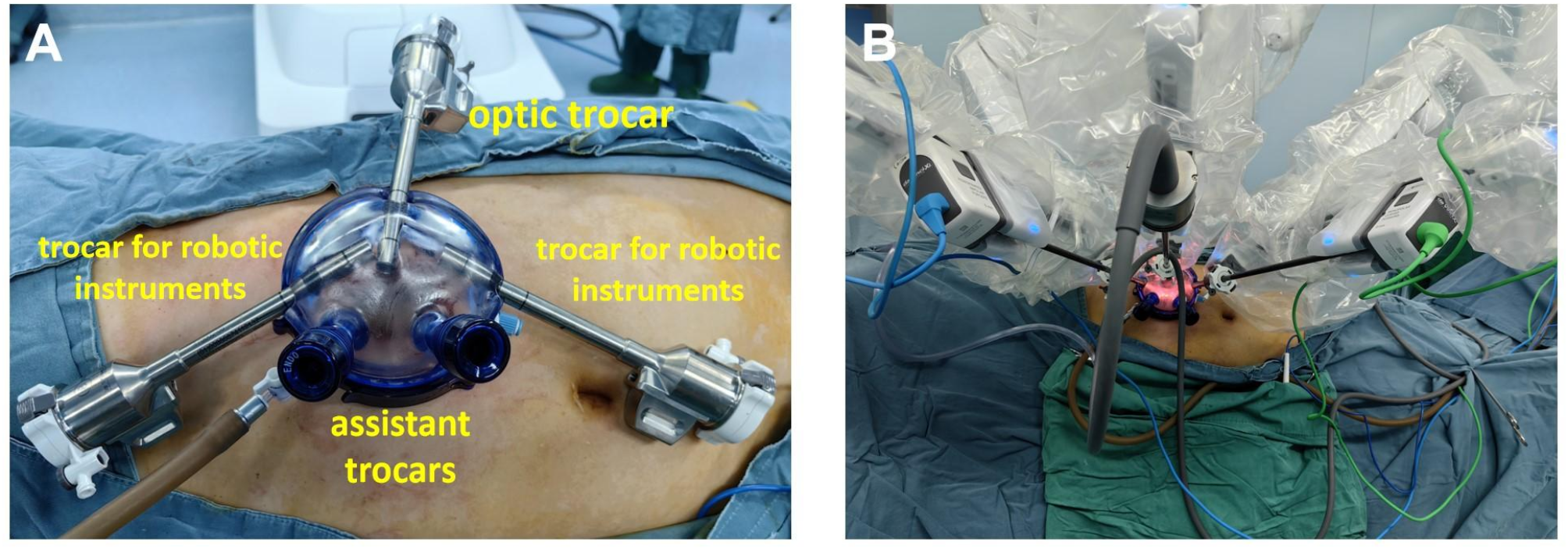
LESS-HPN techniqueAll surgeries were performed using the da Vinci XI Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). After administering general anesthesia, the patient assumed a 70-degree lateral position. Following the open Hasson technique, a 4.5–5.0 cm lateral rectus incision was made on the affected side, and a Freeport (Ningbo SensCure Biotechnology) was inserted. The Freeport was equipped with one 8-mm optic trocar and two 8-mm working trocars, which were positioned at 12 o’clock, 3 o’clock, and 9 o’clock directions, respectively. Additionally, two assistant trocars were placed within the Freeport. (Fig. 1).
Fig. 1
(A) After a Freeport (Ningbo SensCure Biotechnology) was inserted. One 8-mm optic trocar and two 8-mm trocars for robotic instruments were placed at 12o’clock, 3o’clock, and 9o’clock direction, respectively, and two assistant trocars were placed at the same time. (B) da Vinci XI robot was docked
Through the two assistant channels on the Freeport, the monitoring area of the LUS probe was able to cover a large area of abdominal organsand vessels (Fig. 2). After locating the tumor with LUS, the perirenal fat was directly incised to expose the renal tumor border. Unlike conventional PN, the paracolic sulci, most of the perirenal fat, and renal hilum structures did not need to be dissected.
Fig. 2
Through two assistant trocars, the monitoring area of the LUS probe can cover the large intra-abdominal vessels. (A) The LUS was swept to the long axis of iliac vessels through the assistant trocar caudal. (B) Through the assistant trocar caudal, LUS swept the long axis of the abdominal aorta. (C) Through the assistant trocar caudal, LUS swept the long axis of the abdominal aorta and renal artery orifice. (D) Through the assistant trocar cephalad, LUS swept to the long axis of the renal artery
Actually, prophylactic dissection of the renal artery was performed in the first few cases of UBo-HPN, but this proved unnecessary. Therefore, the renal artery was not dissected in any of the subsequent LESS-HPN cases.
Ultrasound-guided femoral artery puncture was performed, and a vascular sheath was inserted. Under full LUS guidance, a catheter and a guidewire were advanced through the femoral vascular sheath into the main, branch, or accessory renal artery. A Fogarty balloon catheter was then placed at the target artery along the guidewire, inflated with saline to occlude the blood supply.
After confirming complete occlusion of the tumor’s arterial blood supply using color Doppler flow imaging (CDFI) or contrast-enhanced laparoscopic ultrasound (CE-LUS), the tumor was routinely excised and the wound was sutured in the conventional manner. The balloon catheter was deflated and withdrawn, and the renal wound was inspected for bleeding. The specimen was extracted through the incision. and a drain tube was placed at its lowest point (Supplementary Fig. 1). Hemostasis at the femoral artery puncture site was achieved using an arterial closure device.
Technical success was defined as the simultaneous achievement of: (i) complete occlusion of arterial blood flow confirmed by CDFI, or CE-LUS, with direct visualization during the following tumor resection and suturing, and (ii) absence of conversion to conventional multiport robot assisted or laparoscopic partial nephrectomy.
All patients received follow-up every three to six months.
Study variablesBaseline information was recorded for all patients. The complexity of tumors was determined with the R.E.N.A.L. score [13]. Intraoperative variables including operation time, warm ischemia time (WIT), estimated blood loss (EBL), blood transfusion, and incision length was recorded. The number of additional access and any kind of conversion were recorded.Intraoperative or postoperative complications were grade according to Clavien-Dindo classification [14].
Patients received follow-up every three to six months in the first two years and then annually.
Statistical analysisCategorical variables were expressed as frequencies and percentages. Continuous variables that conformed to a normal distribution were expressed as mean ± standard deviation (SD). Those that did not fit the normal distribution were expressed as median and interquartile range (IQR). Comparisons between the two groups (anterior vs. posterior location) were conducted using Student t-tests, and comparisons of dichotomous variables were conducted using Fisher’s exact probability method. Two-sided P value < 0.05 was considered for statistical significance.
Comments (0)