
Remember me



Patients suspected of having PCa who underwent pathological examination between 2020 and 2023 at Shanghai Changhai Hospital, Shanghai Shibei Hospital, and Taizhou People’s Hospital were selected. Among these, patients diagnosed with PCa were identified, and those with BPH were screened using an IPSS ≥ 8 and TRUS ≥ 30 ml. The cohort consisted of 89 PCa cases and 198 BPH cases. The extracted patient variables included age, BMI, total prostate-specific antigen (tPSA) in blood, free PSA (fPSA) in blood, and the percentage of free PSA (fPSA/tPSA). Additionally, based on urinary exosome testing, the study incorporated urinary exosome PSA (u-PSA), α-methylacyl-CoA racemase (u-AMACR), and prostate-specific membrane antigen (u-PSMA), along with the quantitative biochemical measurements of u-AMACR, u-PSA, and u-PSMA.
This study strictly adhered to the ethical principles outlined in the Declaration of Helsinki, ensuring that all data were derived from actual clinical cases. Informed consent was obtained from each patient or their legal representative before sample collection. Data inclusion or exclusion was based on the following criteria. Inclusion criteria: (1) Patients diagnosed with PCa or BPH through pathological examination, IPSS and TRUS; (2) Patients who provided sufficient urine samples with quality meeting the requirements for exosome extraction and analysis; (3) Complete routine clinical records; (4) Age ≥ 18 years. Exclusion criteria: (1) Patients who had undergone prostate-related surgery, radiation therapy, or hormonal treatment within three months prior to sample collection; (2) Patients diagnosed with other malignant tumors. The study was approved by the local ethics committee (Approval No.: CHEC2013-115).
Exosome extractionWe collected the first morning urine samples from patients and processed them within 2 h of collection. First, the samples were centrifuged at 3000×g to obtain the supernatant. Following the method from our previous research, exosomes were extracted using a commercial kit (EIQ − 03001 (Urine), Wayne Bio, Shanghai, China). The procedure was as follows: the supernatant was mixed thoroughly with reagent A (7.5 mL) and reagent B (670 mL) and incubated at 4 °C for 12 h. Then, the mixture was centrifuged at 3000×g at 4 °C for 1 h, retaining 1 mL of supernatant and discarding the remainder. The pellet was resuspended in the retained 1 mL supernatant. The resuspended solution was centrifuged at 10,000×g for 10 min, and the supernatant was discarded. The pellet was then resuspended in 200 µL of phosphate-buffered saline (PBS). Next, the sample was centrifuged again at 10,000×g for 5 min. The supernatant containing the exosomes was transferred to a 1.5 mL centrifuge tube (EP tube) and stored at −80 °C. The exosome extraction and identification steps were performed as previously described.
ELISAFirst, the working solution was prepared according to the manufacturer’s instructions. Next, the standard solution was diluted at the same ratio, and either the standard or the sample was added to a 96-well plate pre-incubated with the primary antibody. The plate was incubated in an incubator for 2 h. Afterward, 100 µL of reagent A was added, and the plate was gently shaken for 1 h in the incubator. The wells were washed with 300 µL of wash buffer per well for 2 min. The procedure for reagent B was performed as previously described. Finally, the reaction solution was added to each well and incubated at 37 °C for 15 min. Once a clear color gradient appeared in the standard wells, the reaction was terminated by adding stop solution, and the absorbance was measured at 450 nm. The concentration in the samples was determined and recorded by comparing the optical density of the samples to the standard curve.
Feature selectionTo reduce the number of features tested by different classifiers, feature selection was performed. The dataset contains 287 cases of PCa and BPH, with each case consisting of 11 feature variables. Initially, parameters with no significant differences between the two groups were eliminated. Subsequently, feature selection was conducted using Least Absolute Shrinkage and Selection Operator (LASSO) regression. LASSO regression is a statistical modeling technique that combines variable selection with regularization, making it particularly suitable for high-dimensional data analysis. By adding an L1 regularization term to the loss function, the method enforces sparsity constraints and controls overfitting. We applied a 10-fold cross-validation method for validation, which not only alleviated overfitting due to the repeated use of training and test data, but also optimized the regularization parameter λ (which controls the strength of the Lasso penalty), thus achieving a balance between the number of retained predictor variables and predictive performance. The final selected features were used for subsequent model training and analysis.
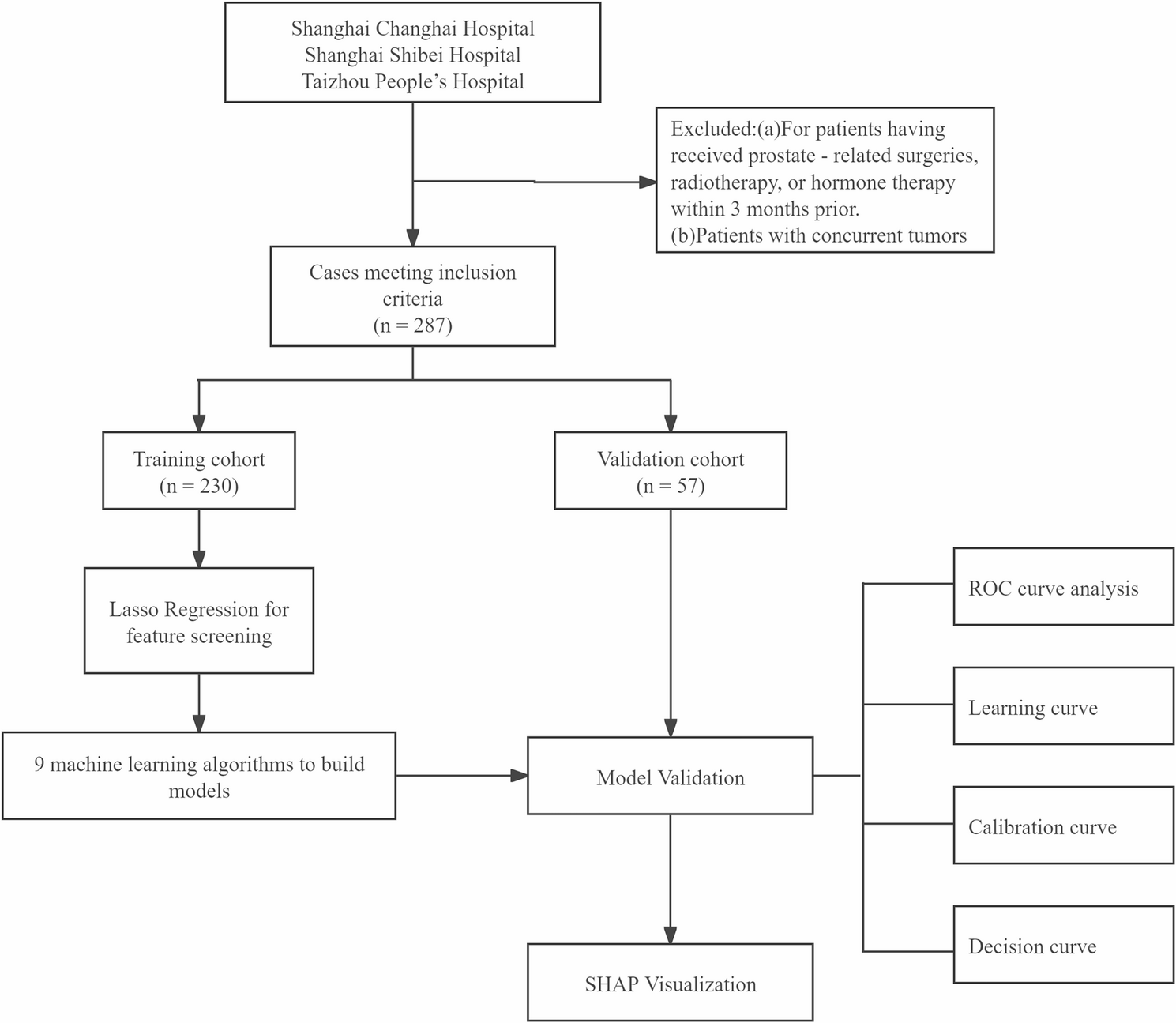
Study designThe workflow of this study is briefly outlined in a flowchart, and a systematic description of the study cohort is provided (Fig. 1). Specifically, retrospective data collected from Shanghai Changhai Hospital, Taizhou People’s Hospital, and Shanghai Shibei Hospital were randomly divided into a training set (n = 230, 80%) and a validation set (n = 57, 20%). Based on the training set data, models were constructed using nine ML algorithms, including Extreme Gradient Boosting (XGBoost), Light Gradient Boosting Machine (LightGBM), Random Forest, Adaptive Boosting (AdaBoost), Decision Tree (DT), Gradient Boosting Decision Tree (GBDT), Gaussian Naive Bayes (GNB), Support Vector Machine (SVM), and K-Nearest Neighbors (KNN). Diagnostic model parameters selected from the training set were used to validate the diagnostic performance of the chosen models. The nine models were then comprehensively evaluated, and the classifier with the best predictive performance was selected to establish the final diagnostic model. Model performance was evaluated using metrics such as accuracy (ACC), negative predictive value (NPV), and positive predictive value (PPV), and further assessed through receiver operating characteristic (ROC) curves, learning curves, calibration curves, and decision curves. Finally, SHAP (Shapley Additive Explanations) was used to demonstrate the impact of feature variables on model outputs.
Fig. 1
Flowchart of the construction of a diagnostic model for prostate cancer using urinary exosomes. ROC, receiver operating characteristic curve
Statistical analysisAll data were statistically analyzed using SPSS Statistics software (version 26.0) and Python software (version 3.4.4). Quantitative data underwent normality testing. Normally distributed data were expressed as means and variances, and analyzed using Student’s t-test. Non-normally distributed data were expressed as medians and interquartile ranges (IQR), and analyzed using the Mann-Whitney U test. Qualitative data were expressed as frequencies and percentages, and analyzed using the chi-square test. All statistical tests were two-sided, and a P-value < 0.05 was considered statistically significant.
Comments (0)