Recent advances in energy and technology have led to the emergence of various new types of transurethral surgical therapies, such as laser, bipolar energy enucleation, or vaporization, and aquablation, which has led to diversified BPH treatment [12]. Although there has been a growing amount of literature reporting on such treatments, the relationship between TUEB and other techniques in the management of BPH remains unclear. One meta-analysis [13] revealed that, compared to TUEB, HoLEP had a shorter catheterization time (p = 0.007), higher operative time (p = 0.03), higher enucleation weight (p = 0.01), and shorter bladder irrigation time (p = 0.01). However, there were no significant differences observed between the techniques in terms of transfusion rates, complications, LOS, or postoperative functional outcomes at 1, 3, 6, 12, or 24 months.
From our point of view, there is a difference in technique between performing HoLEP and TUEB for BPH. Regarding prostate mucosal notation, the position of the mucosa that is indicated in both techniques is similar in that, in both cases, an incision is applied to the area around verumontanum starting at 6 o’clock and heading to the capsular membrane at 12 o’clock. Meanwhile, when performing groove formation at 6 and 12 o’clock, in the case of HoLEP, the prostatic median lobe is enucleated from verumontanum in the direction of the bladder neck, while in the case of TUEB, the median lobe is excised to form a groove, and then also expanded to both sides following resection of the tissue at apex in 12 o’clock. Regarding surgical plane formation and enucleation, in HoLEP, it is easy to form the surgical plane due to the vibration of the laser; meanwhile in TUEB, it is easy to find a plane using a resectoscope or loop as if one is using a broom. When dealing with prostatic apex, in HoLEP, the incision started from 12 o’clock and was pushed down to both sides with a laser, but in TUEB, the hanging tissue is cut off with a cutting current. Regarding hemostasis, in HoLEP, the laser is irradiated until hemostasis occurs by stopping at the bleeding focus, but in TUEB, immediate hemostasis is easy using the loop at the same time of enucleation. Finally, when removing peeled tissue, in HoLEP, morcellation is performed and the remaining tissue in the fossa is cut off with a laser; by contrast, the tissue can be cut off by the loop as well as morcellation in TUEB [14]. It is ultimately concluded that HoLEP is definitely advantageous for surgical plane formation and tissue incision during the enucleation process [15], but that TUEB has more advantages for hemostasis and tissue removal after enucleation, thus providing a wide range of options [16]. Another network meta-analysis [17] showed that TUEB appeared to have superior efficacy compared to monopolar TURP and open prostatectomy in BPH with volume > 60 cc. The bipolar energy system can effectively reduce the pressure in the bladder, relieve bladder outlet obstruction, and restore the physiological function of the bladder detrusor muscle, ultimately improving urination function [17, 18].
One of the most prominent aspects of our findings is that the enucleation efficacy increased along with chronological time. This parameter is expressed as a simple fraction consisting of a numerator (enucleated weight) and a denominator (enucleation time), and this ratio was found to be increased in the ‘Late group’. This indicates that the surgeon can successfully enucleate more adenoma as they accumulate surgical experience. A prior study conducted by a single surgeon [3] suggests that TUEB has a steep learning curve, but that its effectiveness increases significantly after 50 completed procedures. In line with this finding, the rate of reoperation due to bleeding and conversion to TURP was also decreased. With accumulated operation cases, it is expected that a surgeon’s skills in hemostasis will become more sophisticated to achieve better bleeding control and a clearer operative field to reduce reoperation and technique conversion. In the subsequent follow-up cohort of patients analyzed in this study by the same surgeon, the efficiency of enucleation was evaluated according to prostate volume size. The results demonstrated that enucleation efficiency increased with increasing prostate volume (Prostate volume < 40 cc, 40-80 cc, & ≥80 cc: 0.36, 0.44, & 0.73 g/min, respectively) [19]. Furthermore, no significant differences were observed in functional outcomes or complications. These findings might be attributed to the superior hemostatic properties of the loop utilized during TUEB.
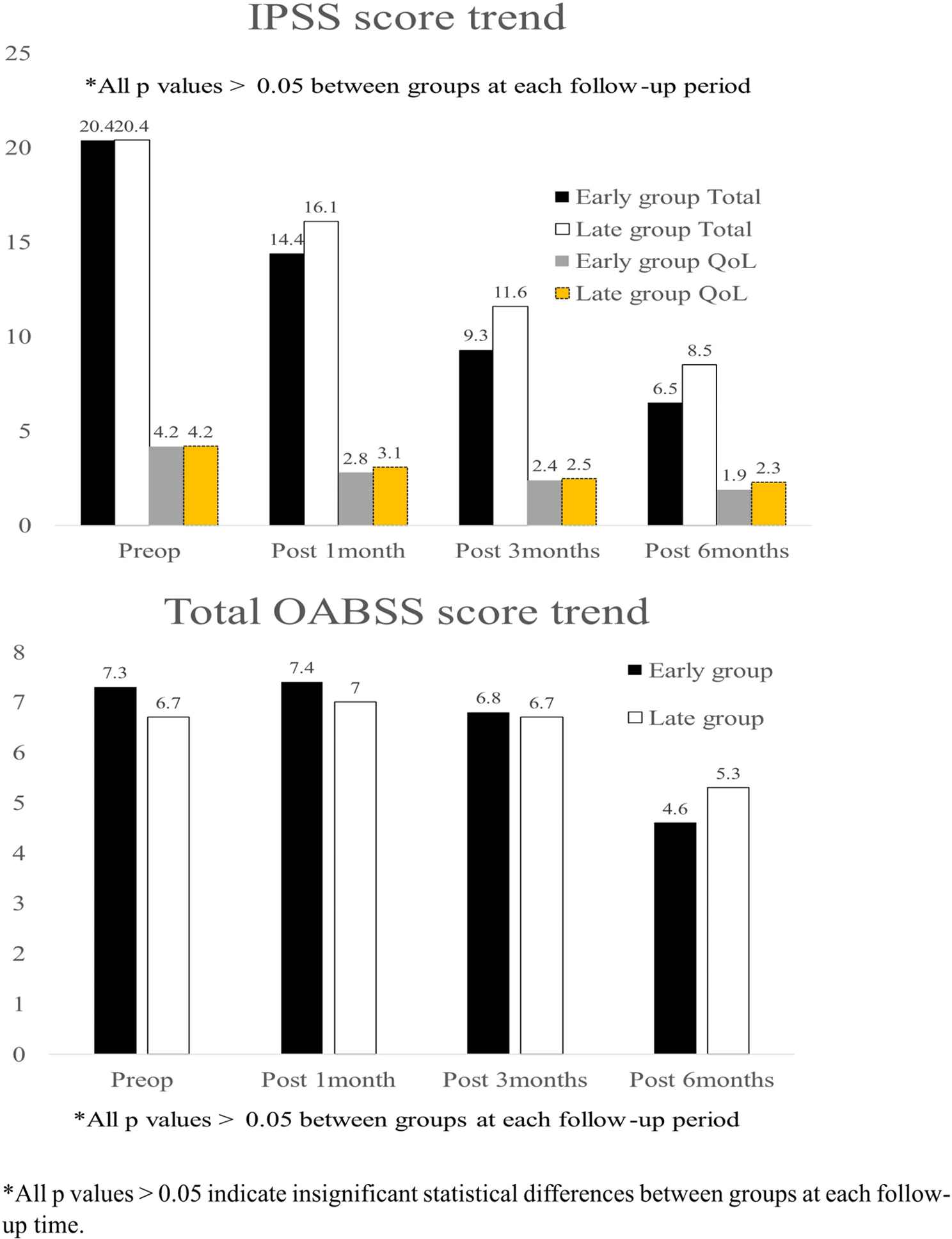
Nevertheless, some of our findings require further elucidation and detailed interpretation. First of all, as a surgeon with over 300 HoLEP procedures and also comparable number of conventional TURP procedures (relative more familiar and faster technique than TUEB), there might be little delay in decision-making regarding the conversion to TURP, which may have resulted in prompt conversion to TURP in real clinical operation field. Therefore, total operation time difference between the groups might not be significant. Secondly, prolonged LOS cases were observed in our cohort. One of the reasons for prolonged LOS was some patients’ personal circumstances, such as a desire to restart anticoagulants during the hospitalization. In the majority of other cases, the hematuria did not sufficiently improve to warrant decatheterization and discharge from the hospital. Thirdly, there was no significant difference in total OABSS questionnaire score between preoperative, postoperative 1 & 3 month. A study [20] revealed that older age was associated with a slower decline in total OABSS questionnaire score following HoLEP. Furthermore, a study reporting the outcomes of 3,000 South Korean HoLEP patients [21] did not report a statistically significant difference in the reduction of total OABSS scores at postoperative two weeks and three months compared to the baseline. These findings are believed to be applicable to ours in that we evaluated outcomes after enucleation technique, although different type of energy was used. Finally, our study showed relatively small resected weight compared to others [1, 13]. this result can be related to the surgeon’s learning curve. In our previous study [22], 70 cases will make comparable efficiency of TUEB and a systemic review [23] reported that TUEB requires approximately 40 cases to 50 cases to overcome learning curve. One recent multicenter study only needs twenty cases to achieve acceptable outcome of bipolar enucleation [24]. Notwithstanding the relatively modest resected weight, there was a significant improvement in enucleation efficiency (enucleated tissue weight per time unit) in the late group. Although those literature indicates that cases needed to achieve proficiency might vary according to level of experience, TUEB is a relatively straightforward technique that can be mastered in a few dozen, not hundreds, of cases, making it easily feasible to a broad range of surgeons. One of our findings is that there was a significant difference in the distribution of CD grades. This may be attributed to the explanation that as experience was gained, the proficiency in controlling bleeding improved, which subsequently led to a reduction in postoperative complications related to hematuria. Also, significant difference in the rate of CD grade I might be due to the relatively higher number of cases with urinary retention, in the late group, without hematuria than cases with hematuria and urinary retention.
The present study is not devoid of limitations that must be noted. The first is the retrospective nature of the study, although we set up a prospectively maintained database, which was then analyzed retrospectively. Moreover, the lack of randomization could be another limitation; however, there were no significant differences found between the groups, so this bias was likely minimized. Another important limitation of our study is the narrow application of TUEB’s learning curve to other cohorts. As the single surgeon performed over 300 cases of HoLEP before initiating TUEB, the case number needed to overcome the learning curve might be less than the expected number, although this was not fully evaluated in the current study. Another limitation is that the grouping of total patients was arbitrary, as they were classified into the first half and the second half by the chronological date of their surgery. This might not reflect the exact timing of overcoming the learning curve. Meanwhile, in order to minimize the impact of BPH complications on the surgical outcome, our analysis was limited to patients with uncomplicated voiding problems, without complications or underlying medical conditions, or whose medications for BPH were ineffective. This might differ from the methodology employed in other studies that have included patients who underwent surgery due to complications of BPH. Also, there was some follow-up losses. Although there was no follow-up loss at postoperative 1 month, 30 patients were lost to follow-up at postoperative 3 months (Early group: 4 patients & Late group: 26 patients). At postoperative 6 months, 96 patients were lost to follow-up (Early group: 52 patients & Late group: 44 patients). Moreover, the limited sample size for CD grade I and II in each group necessitates a cautious approach to the interpretation of the statistical significance observed in the comparison of CD grades. It is important to recognize that these findings may not necessarily translate into clinical significance. Lastly, as this is a single-center single surgeon series with a relatively short follow-up period, physicians should be cautious when applying our experience to their own cohorts.




Comments (0)