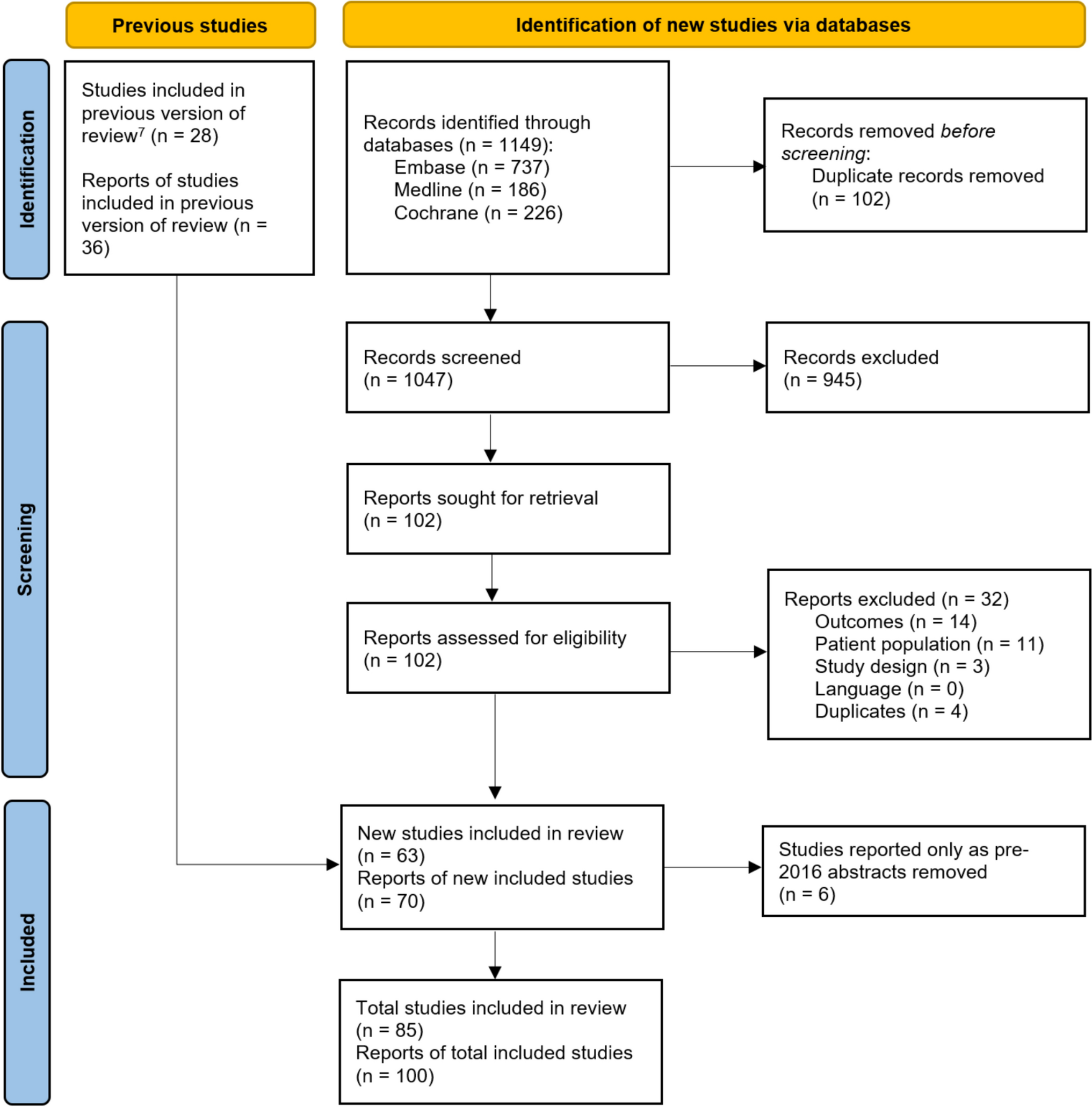
The initial search retrieved 172 records (124 from PubMed and 48 from the Cochrane Library). After removal of 12 duplicates, 160 records were screened for eligibility. One hundred and twenty-two were excluded during abstract screening, and one report could not be retrieved, leaving 37 articles for a full-text review. Following a full-text assessment, 11 articles did not meet the inclusion criteria and were excluded, resulting in 26 studies being retained. A supplementary search strategy—by examining the references of included studies, reviewing relevant organizational websites, and performing citation tracking—identified an additional ten studies, resulting in a total of 36 included studies. The selection process is illustrated in the PRISMA flow diagram (Fig. 1).
3.1 Characteristics of Studies
The included studies demonstrated generally good reporting quality according to the modified CHEERS checklist. Most studies clearly reported study perspective, model structure, population characteristics, comparators, time horizon, discount rates, and main economic outcomes. A detailed summary of the assessed domains for each study is provided in Table 3.
3.1.1 Perspective
Most studies adopted a payer-based perspective (n = 30 [83.3%]), with others using societal (n = 6 [16.7%]). No studies reported results from more than one analytic perspective. For descriptive purposes, perspectives were grouped using the terminology reported by study authors, with payer-based perspectives (e.g., healthcare system, social services, third-party payer, insurer) summarized together, as they are conceptually similar.
3.1.2 Country
Geographically, analyses were conducted mainly in Asia (n = 14 [38.9%]), Europe (n = 12 [33.3%]), and North America (n=7 [19.4%]), with only one study from South America (n = 1 [2.8%]), and two were conducted in two or more continents (n = 2 [5.6%]). No studies were identified from low-income countries.
3.1.3 Model
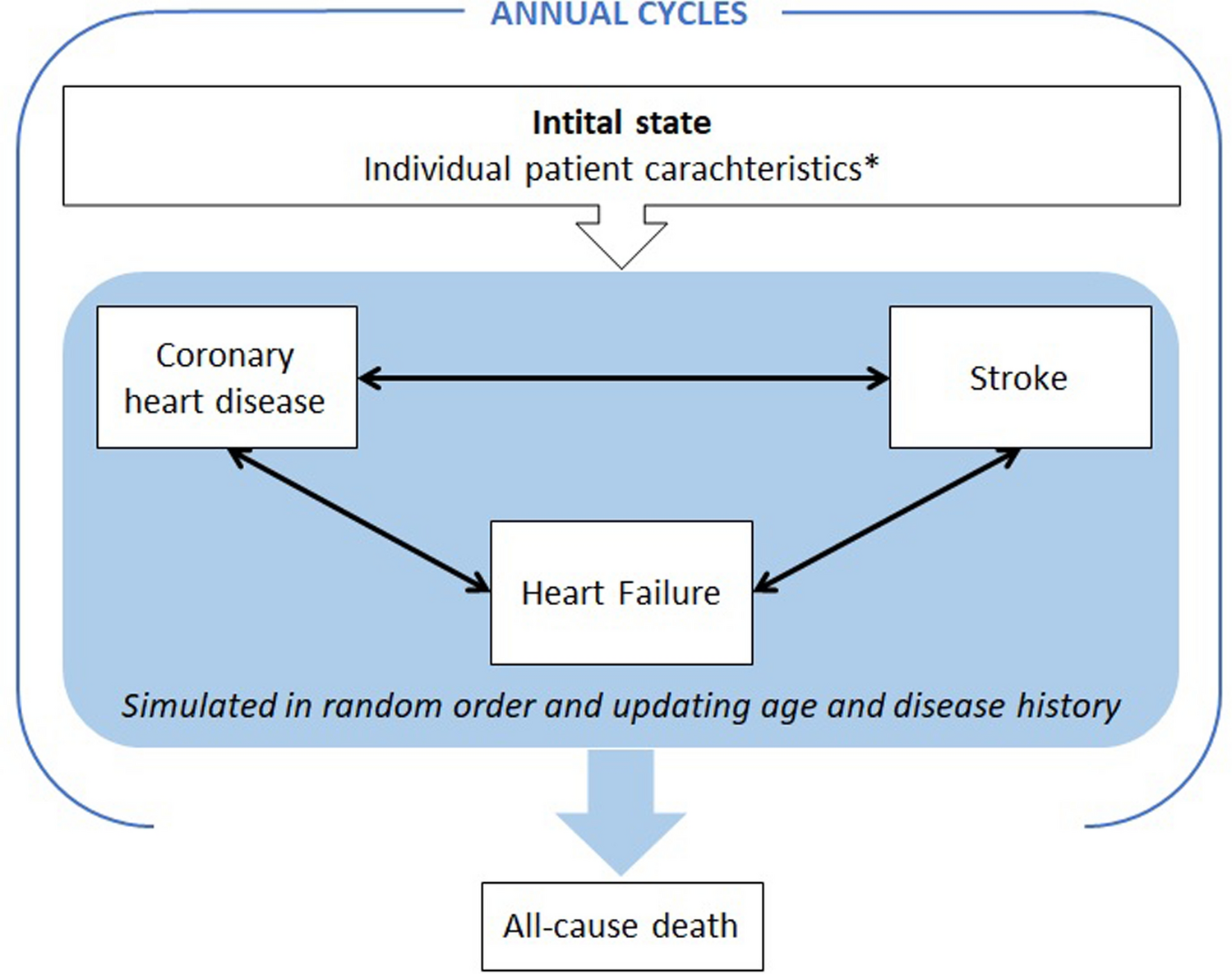
Most evaluations employed Markov or microsimulation models to simulate patient cohorts progressing through CKD stages until death, accounting for common comorbidities such as type 2 diabetes mellitus (T2DM) and cardiovascular disease. Most models relied on structured frameworks such as DAPA-CKD, FINE-CKD, or CREDEM-DKD cost-effectiveness models [20, 54, 55] and clinical trials (n = 33 [91.7%]). One study applied two separate Markov models for diabetic versus non-diabetic cohorts (n = 1 [2.8%]) [43], another used shared-parameter models (n = 1 [2.8%]) [40], and one used a discrete event simulation (n = 1 [2.8%]) [49].
3.1.4 Medication
Studies assessing SGLT2i included canagliflozin (n = 4 [11.1%]), empagliflozin (n = 11 [30.6%]), dapagliflozin (n = 13 [36.1%]), and sotagliflozin (n = 1 [2.8%]); three studies did not specify the SGLT2i intervention (8.3%) [47, 50, 53]. Finerenone was evaluated in eight studies (22.2%), all in patients with CKD with T2DM. Comparators were most frequently SoC (typically ACE inhibitors, angiotensin II receptor blockers, and other concomitant therapies, though some studies did not provide details on the SoC applied) or placebo; notably, the sotagliflozin study compared its cost effectiveness with insulin monotherapy [41]. Finally, vadadustat and sparsentan were each assessed in one study (2.8%), compared against darbepoetin alfa and irbesartan, respectively [38, 39].
3.2 Cost per CKD Stage3.2.1 Stages 1–2
Direct costs associated with CKD rise progressively with advancing disease severity, although estimates varied substantially across studies, countries, and analytic perspectives. In early CKD (stages 1–2), costs were generally low but showed wide cross-country variation. For example, annual expenditures ranged from $98 in Canada [27] to $25,104 per patient per year in the USA [41]. Some evaluations reported minimal differences between stages 1 and 2, while others showed modest increases up to 1.4-fold [23, 33], reflecting differences in healthcare utilization and study design.
3.2.2 Stage 3
A more pronounced escalation in costs was consistently observed, beginning in stage 3, coinciding with greater healthcare resource use and the onset of more frequent complications. An English study reported an 8.3-fold increase in annual direct costs per patient from early stages to stage 3 [18]. Some studies further subdivided this stage: costs in stage 3b were notably higher than 3a, with a range from modest differentials (1.06-fold in Malaysia) to more substantial increases (3.5-fold in France) [31, 33, 35]. These differences highlight the clinical and economic importance of disease progression even within moderate CKD.
3.2.3 Stage 4
Progression to stage 4 was generally associated with further increases in direct costs, although heterogeneity remained high. A Canadian study described a moderate rise compared with stage 3, from $211 to $378 annually (a 1.8-fold increase) per patient [27], whereas a study in China reported flat costs across stages 1–4 ($132 per year) [37]. Despite these discrepancies, stage 4 consistently represented a transition point to more intensive resource use and preparation for KRT.
3.2.4 Stage 5
Stage 5, particularly before the initiation of dialysis, was associated with some of the most pronounced cost increases. The largest increases were reported in Canada, where direct costs per patient rose from $378 per year at stage 4 to $5353 per year at stage 5 without dialysis (a 14.2-fold increase) [27], and in China, where costs increased from $132 per year in earlier stages to $891 at stage 5 (a 6.7-fold increase) [37]. A few studies do not reported differences between stages 4 and 5, such as cost estimates of $9528 per year in the USA (without transplant) [22] and $2876 per patient per year in Vietnam [33], underscoring again the substantial influence of setting and perspective on absolute costs.
3.2.5 Dialysis and Kidney Transplantation
The most significant cost burden emerged once patients had initiated dialysis or underwent kidney transplantation. Dialysis costs ranged widely, from $35,581 per year for peritoneal dialysis to $70,539 for hemodialysis in France [31], while national differences were stark. For example, estimated annual dialysis costs were $57,078 in the UK, $88,675 in Germany, and $69,674 in Spain [20]. Transplantation also involved high initial costs: $80,475 in the first-year post-transplant in Canada, decreasing to approximately $25,000 annually thereafter [27]. These findings confirm that KRT constitutes the dominant driver of CKD-related healthcare expenditures.
3.2.6 Other Factors
In addition to eGFR-based staging, other clinical factors contributed meaningfully to cost variability. High levels of albuminuria or elevated urine protein-to-creatinine ratio, which are markers of kidney damage, were consistently associated with higher costs [28, 39], as were comorbidities such as T2DM and cardiovascular disease. Treatment-related adverse events also played a significant role and were incorporated into several cost-effectiveness model structures. A summary of costs by CKD stage and KRT is presented in Table 4.
3.3 Cost Effectiveness of Drugs for CKD3.3.1 SGLT2i
According to the included studies, SGLT2i (dapagliflozin and empagliflozin) were the most frequently evaluated therapies in CKD populations [20,21,22,23, 26, 28, 30,31,32,33,34,35,36, 38,39,40, 43, 44]. All studies reported QALY gains relative to SoC.
Over long-term horizons of 20 years or lifetime, incremental QALYs generally ranged from 0.2 to 1.31 [20,21,22,23, 26, 28, 30, 31, 33,34,35,36, 44], whereas shorter-term analyses (2–10 years) showed smaller gains, from 0.012 at 2 years [40] to 0.23–0.457 at 10 years [32, 43].
Cost outcomes for SGLT2i varied substantially across countries. Seven of 16 studies found treatment to be cost saving [23, 26, 28, 30, 31, 34, 35], with the largest savings reported in the Netherlands ($40,117) [30]. Cost saving was also reported in Malaysia and Thailand but not in Vietnam, where the estimated ICER was $3690 [33]. Higher incremental costs appeared in high-income settings, particularly the USA, where one study estimated incremental costs of $100,330 [22].
Baseline CKD severity influenced cost effectiveness. A Japanese analysis showed markedly different ICERs depending on CKD stage: $1311 for stage 3b and $44,016 for stage 3a, driven by larger risk reductions in more advanced disease [21]. Two multi-national evaluations of dapagliflozin reported favorable lifetime ICERs across high-income countries: $9936 (UK), $21,148 (Germany), and $14,024 (Spain) in one study [20], and $11,850 (UK), $16,072 (Spain), $8626 (Italy), and $15,233 (Japan) in another [36]. Other lifetime evaluations estimated ICERs of $76,200 in the USA [22] and $3846 in Thailand [44]. At 10 years, incremental costs were $1372 in Colombia and $1939 in Japan, with ICERs of $5956 and $4245, respectively [32, 43]. A 2-year multi-country analysis found incremental costs of $341 and an ICER of $29,422 [40].
3.3.2 Other Drugs
Evidence for non-SGLT2 therapies was more limited and only available in the UK. Vadadustat gained 0.03 QALYs at an incremental cost of $1095, producing an ICER of $43,303 [38], while sparsentan showed an ICER of $329,038 versus irbesartan at the list price, falling dramatically to $38,804 under a patient access scheme [39]. Complete economic outcomes are summarized in Table 5.
3.4 Cost Effectiveness in Patients with CKD and Diabetes3.4.1 SGLT2i
Among studies focused on CKD in patients with diabetes, mainly T2DM, QALY gains were consistently reported across all therapies evaluated [18,19,20, 24, 25, 27, 29,


Comments (0)