
Remember me
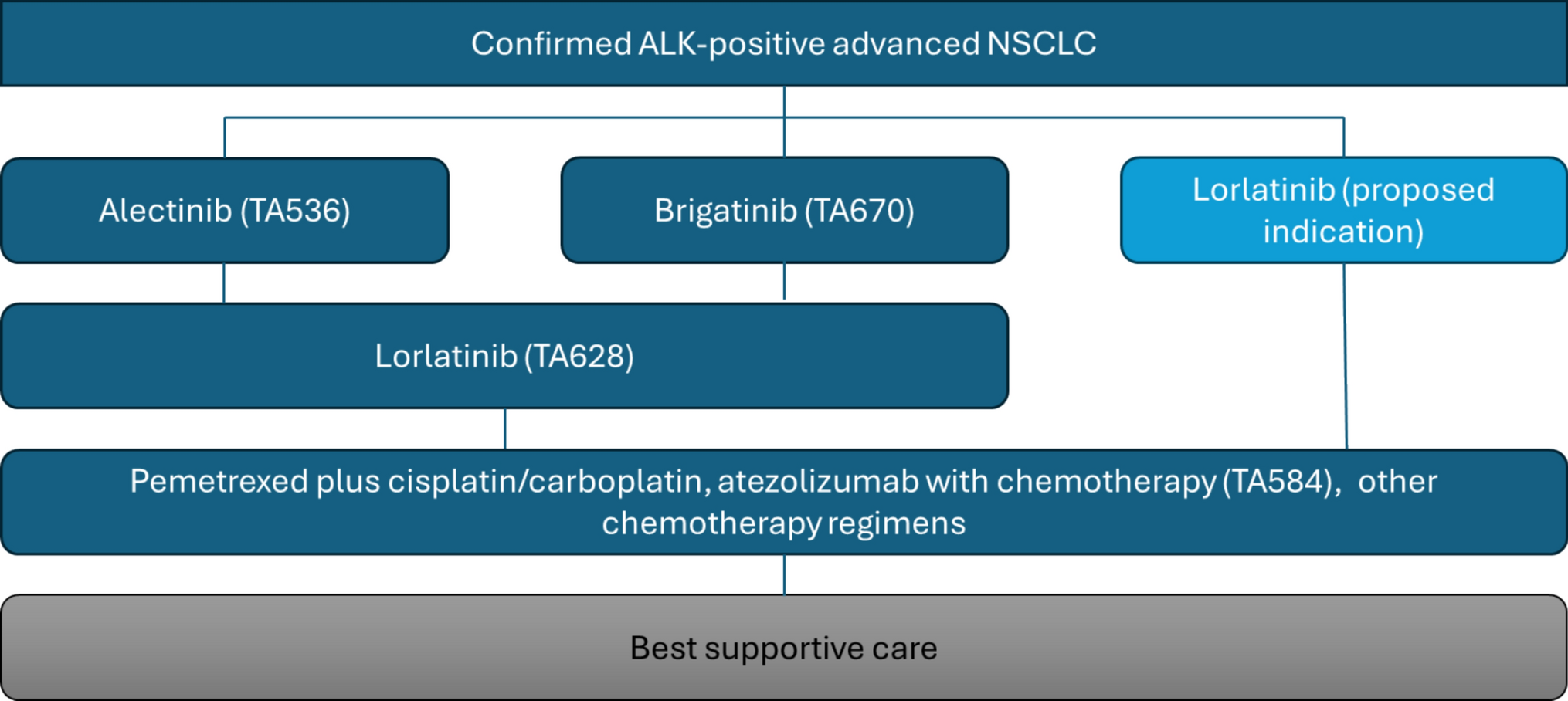

NICE invited Pfizer to submit evidence on the clinical and cost effectiveness of lorlatinib for previously untreated ALK-positive advanced NSCLC. The comparators defined in the NICE scope were alectinib and brigatinib, both standard first-line treatment options in the NHS. Lorlatinib is already recommended by NICE (TA628) [4] for patients with previously treated ALK-positive advanced NSCLC and is currently used in the NHS as a second-line treatment option alongside pemetrexed-based chemotherapy, see Fig. 1.
Fig. 1
Proposed positioning of lorlatinib in the clinical pathway. ALK anaplastic lymphoma kinase, NSCLC non-small-cell lung cancer
As indicated in Fig. 1, if lorlatinib were recommended in the first-line setting, patients would no longer have access to other ALK inhibitors in the second-line setting, leaving pemetrexed-based chemotherapy as the only subsequent treatment option. Consequently, the company’s decision problem can be conceptualised as a comparison of alternative treatment sequences, including scenarios in which lorlatinib is reserved for use after either alectinib or brigatinib.
In the second-line setting, the NICE recommendation for lorlatinib was subject to a simple PAS discount. For the first-line appraisal, Pfizer proposed a revised conditional PAS, larger than the existing second-line discount. However, the availability of this larger discount was contingent on a positive first-line recommendation. The conditional PAS offered by Pfizer was not indication specific; as such, approval of lorlatinib for first-line use would mean that the revised (conditional) PAS applies across both first- and second-line indications.
To capture this conditionality in the economic analysis, the company applied the conditional PAS to first-line treatment while retaining the existing PAS for second-line use. This approach sought to represent the world as it is currently in the comparator arm while representing the counterfactual world in the intervention arm.
Comments (0)