
Remember me
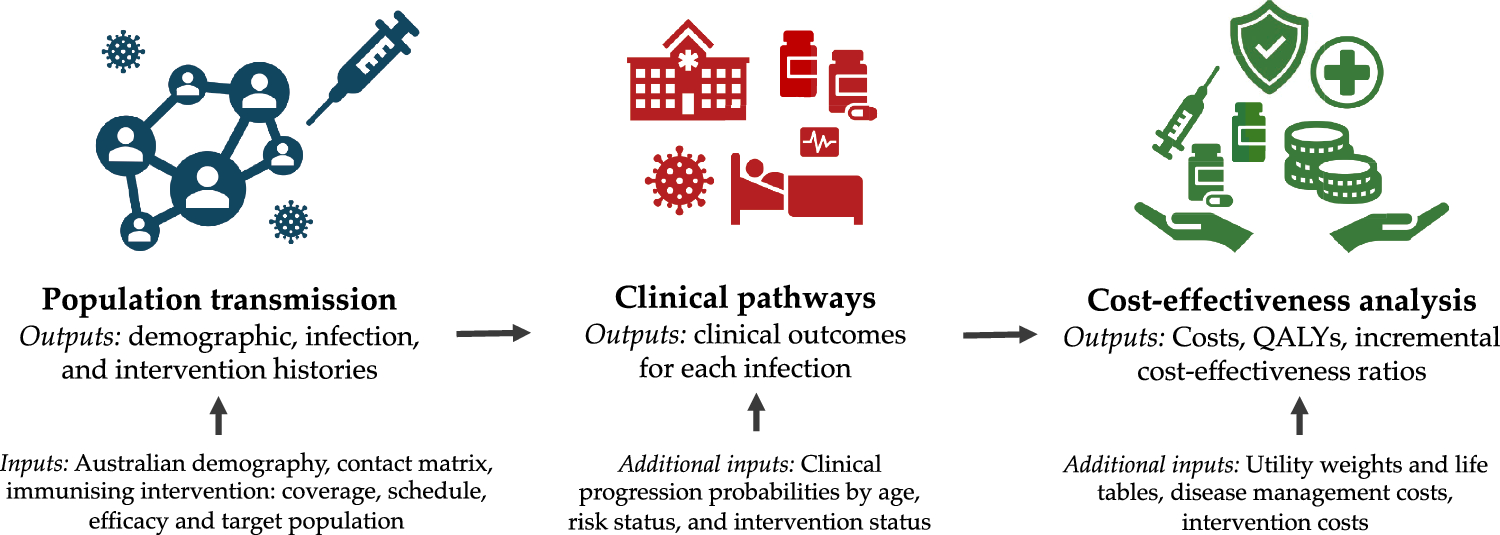

We estimated the cost-effectiveness of different programs of immunisation products, via a pipeline of three distinct models. These models, as shown in Fig. 1, were (i) a transmission model of epidemic spread and immunisation product roll-out, (ii) a clinical pathways model that probabilistically simulated clinical endpoints given an infected individual’s age, risk status and immunisation status, and iii) a cost-effectiveness model that computed incremental costs and quality-adjusted life-years (QALYs) compared with the no-intervention scenario.
Fig. 1
Schematic overview of the inputs and outputs of the transmission, clinical pathways and cost-effectiveness models
2.1 Infection and Transmission Model OverviewThe goal of the population transmission model was to reproduce key trends of RSV infection in Australia and to project likely transmission dynamics given introduction of different combinations of immunisation products.
The transmission model was a dynamic individual-based model. We tracked the age (to the granularity of days), sex, age at death, and the demographic status of each individual. We explicitly modelled pregnancy and connected infants and pregnant people. We matched to Australian data for the age-sex distribution, age- and sex-specific mortality rates, fertility rates and the gestational age of newborns upon birth. The simulated population of 100,000 individuals included a birth cohort per year of roughly 1300 infants, matching Australian demographic data. We assumed age-stratified population-level mixing of individuals as estimated for the Australian population by Mistry et al. [10]. Details on demographic data sources and simplifying choices are outlined in Appendix A in the supplementary materials.
The model assumed that repeated exposures over the life course of an individual build natural immunity to infection with RSV. We did so via a tiered susceptible-exposed-infectious-recovered-susceptible (SEIRS) model of RSV infection, where after recovery following infection, subsequent infection is less likely. This compartmental structure is commonly used for RSV models [11, 12]. Further mathematical details of the transmission model are in Appendix B in the supplementary materials.
Given limited Australian data on the incidence of RSV in settings other than hospitals, we calibrated the uncertain parameters of the transmission model and the probability of hospitalisation given infection to historical RSV-coded hospitalisation data (2018–2019) provided by the Department of Health, Disability and Ageing using Admitted Patient Care data supplied by the Australian Institute of Health and Welfare (AIHW). We also ensured the infection dynamics were consistent with the accepted heuristic that 75% of infants are infected with RSV in their first year of life, and 95% by 2 years of age [13, 14]. We used hospitalisation data from 2018 to 2019 given clear coronavirus disease 2019 (COVID-19) impacts on RSV circulation in Australia from 2020 to 2022, and because data were not available beyond 2022. The data sources and further details of model calibration are in Appendix C in the supplementary materials.
We used a dynamic, individual-based transmission model for two main reasons, despite little assumed protection against acquisition of infection or onwards transmission conferred by MV or mAbs (see Sect. 2.3). One, this model structure allowed for explicit connections between pregnant persons and infants, to capture the dependence of infant protection on that of their mother (see Section B.4 in the supplementary materials). Two, the model structure enabled a rapid, iterative, participatory approach in model and scenario development with ATAGI and the Department of Health, Disability and Ageing, as the policy landscape was evolving in 2024 in Australia.
2.2 Clinical Pathways Model OverviewThe model had six mutually exclusive clinical endpoints for each RSV infection that were directly relevant to healthcare costs. As shown in Fig. 2, these endpoints were: no medical care sought, general practitioner visit (GP), emergency department consultation with no admission to a hospital ward (ED), admission to a hospital ward (hospitalisation) without further progression, admission to an intensive care unit (ICU) and death following admission to an ICU (death).
Fig. 2
Flowchart illustrating the clinical pathways model
We mapped infections to clinical endpoints in an age- and risk-specific manner, using Australian data wherever possible. We probabilistically assigned only the final clinical outcome experienced for each RSV infection, assuming that medically-attended RSV infections progress sequentially through the clinical pathway. For example, we assumed that an individual who is assigned a clinical endpoint of ICU previously presented to the emergency department and was admitted to a hospital ward. Similarly, we assumed that fatalities only occur following admission to ICU. Given limited population uptake we did not explicitly assume any impact of short-acting monoclonal antibodies (palivizumab) in the population-level data to which we calibrated the clinical pathways model.
The data used to calibrate the incidence of severe outcomes from the clinical pathways model were National Admitted Patient Care data (i.e. line by line unit records), collated by the Australian Institute of Health and Welfare (AIHW) and supplied to the Department of Health, Disability and Ageing, who aggregated the data by month-of-age and month of the year for the (1) number of infants who are admitted to hospital; (2) the number of infants who are admitted to ICU, and (3) the number of infants who die, after being admitted to hospital. These data are collated nationally across all Australian hospitals. All numbers are for coded hospitalisations with International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD10AM) codes for principal diagnoses (J21.9) and principal or additional diagnoses (J12.1, J20.5, B97.4, J21.0). These data inform age-specific probabilities for all six of our clinical outcomes as smooth functions of age; see Appendix D of the supplementary materials.
Premature infants born prior to 37 weeks’ gestational age were assumed to have a higher risk of severe outcomes (“at-risk”) than infants born after 37 weeks of gestation (“not at-risk”). We used individual-level data of age, risk-status, and clinical outcome in 2017–2019 from a large, tertiary paediatric hospital in Melbourne to estimate the relative risk (RR) for hospitalisation and ICU admission (for an at-risk infant compared with a not at-risk infant) as 2.46 and 5.69, respectively. These data were selected to align temporally with our national hospital admission data (2018–2019) as closely as possible. These estimates aligned broadly with those reported from another Australian paediatric hospital (2015–2022) [15]. In the absence of data from other clinical settings, we assumed the RR for general practice and emergency department visits was equal to the RR for hospitalisation, and the RR for fatality was equal to the RR for ICU admission. Given limited local evidence on the prevalence and relative risk of RSV outcomes for underlying clinical conditions other than prematurity, no other at-risk conditions were explicitly included in our model.
Further details of the clinical pathways model, including data sources and assumptions, are in Appendix D in the supplementary materials.
2.3 Immunisation EfficacyEvidence from clinical trials and early post-licensure observational studies demonstrated that both mAbs and MV prevent severe medically attended disease outcomes in infants [4,5,6, 16,17,18,19,20]. However, the reported clinical efficacy and effectiveness endpoint estimates from studies of each product (e.g. efficacy against lower respiratory tract disease with two or three symptoms) did not map directly to our endpoints of interest, which instead relate to healthcare utilisation given RSV infection. Considering all available evidence, we determined in consultation with ATAGI a set of immunisation efficacy values to use as initial values in the model for both MV and mAbs, and for not-at-risk and at-risk infants. We assumed a general trend of increasing protection with increasing severity of clinical endpoint, ensuring reasonable alignment with the magnitude of efficacy estimates from the trials that mapped most closely to our endpoints. Given the absence of evidence on immunisation efficacy of both products against infection, we ascribed minimal efficacy for this endpoint. The initial efficacy for each endpoint used in the model is included in Table 1.
Table 1 Initial efficacy against infection and clinical endpoints for mAbs and MV, for both at-risk and not-at-risk infantsIn each scenario we modelled, mAbs were only given to newborns and MV was provided to pregnant people between 28 and 36 weeks of gestation. The benefits of MV were only considered conferred to newborns born at least 2 weeks after the vaccination. We assumed that the mAbs immunisation efficacy is at a maximum for 90 days, and the protection wanes exponentially thereafter, with a half-life of 70 days from that point [6, 21]. For MV, we assumed the immunisation efficacy is at a maximum for 90 days post-vaccination, and the protection wanes linearly to zero in the 180 days hence [4]. In the model, the complement of the product specific efficacy against each endpoint at the time of an individual’s infection was multiplied by their age- and risk-specific probability of that endpoint (see Sect. 2.2), to further reduce the probability of each clinical endpoint. These assumptions are further outlined in Appendix D in the supplementary materials.
2.4 ScenariosWe modelled the impact of immunisation programs involving only mAbs (single dose), only MV and programs involving combinations of mAbs and MV.
We assumed mAbs were only delivered to newborns for two reasons: i) the bulk of the disease burden is seen in infants under 4 months of age, and ii) given logistical and programmatic considerations that real-world implementation is most likely to be in a hospital setting prior to discharge after birth of the infant, as part of a suite of products given to infants. For mAbs-only programs, we explored the impact of varying eligibility by at-risk status, as well as the timing and duration of delivery and uptake coverage. We considered both a year-round and a seasonal program, and considered coverage rates of 50% and 70%. A “seasonal” program was defined as February–July to maximise the potential impact, without compromising the efficiency of the overall program. A seasonal program over these months helped to ensure the bulk of the uptake of mAbs (when they are at their highest efficacy) was just prior to and during a typical RSV season. We explored alternative durations and timings for seasonal delivery in Appendix E in the supplementary materials.
For MV immunisation programs, we only explored the impact of varied coverage levels. Seasonal MV programs were not considered feasible in the Australian context: maternal vaccine programs for other diseases are offered year-round [22], thus a different recommendation for RSV would be inequitable and logistically challenging.
Combinations of mAbs and MV were also explored with varied coverage and eligibility. These programs were explored as likely “feasible” programs, that aimed to maximise protection of infants while minimising the use of the more-expensive mAbs (compared with MV). Combination scenarios explored the likely benefit of selectively administering mAbs to newborns not considered protected from MV (on the basis of date of MV delivery and/or gestational age).
Each program’s impact on clinical endpoints was assessed over a 2-year time horizon, by comparing with a no-intervention scenario, that is, a scenario without delivery of either immunisation product.
2.5 Cost-Effectiveness Model OverviewA cost-utility analysis was conducted to evaluate the cost-effectiveness of each program from a healthcare system perspective following national guidelines [23]. Note that this analysis was performed independently of national cost-effectiveness analysis conducted by the Pharmaceutical Benefits Advisory Committee (PBAC). We present results as an incremental cost-effectiveness ratio (ICER), representing the incremental costs per QALY gained compared with no intervention, as per national guidelines. We also perform a sequential analysis to compare each scenario with the next most costly scenario in sequence to identify non-dominated strategies on the cost-effectiveness frontier (see Appendix H). The economic model uses outputs from the clinical pathways model described above, ensuring consistency in the relevant demographics, infection history, immunisation characteristics and infection-related outcomes.
The economic analysis only considered medically attended clinical outcomes in infants over the 2-year time horizon, with QALY losses due to premature mortality captured over a lifetime. QALY decrements were estimated as detailed in Appendix F.2 in the supplementary materials. Briefly, health-related quality-of-life decrements for each clinical outcome were sourced from Shoukat et al. [24] and the duration of each health state was based on length of stay data from the National Hospital Cost Data Collection (NHCDC) dataset [25]. Programmatic costs (dose and administration costs) and costs of healthcare for medically attended cases were included. The dose prices for MV and mAbs in Australia are unknown. We assumed prices of A$290 for mAbs and A$160 for MV in the primary analyses on the basis of U.S. pricing [26], scaled down by 43.6% to reflect reported average difference in medicines prices between the USA and Australia [27]. These estimated prices were varied in sensitivity analyses on the basis of prices reported in the literature in other settings, or used in cost-effectiveness analyses in Australia and elsewhere. A wastage rate of 5% was assumed for both. The cost of dose administration and outpatient visits for non-admitted cases requiring a GP consultation were based on Medicare Benefits Schedule pricing. The cost of outpatient ED visits and hospitalisations were based on the NHCDC dataset. The full details of how costs were estimated are included in Appendix F.3 in the supplementary materials.
Clinical outcomes data were aggregated into 1-year age groups for the economic model. Costs and QALY decrements for illness were assumed to be constant across age groups, while QALY decrements for death were age-specific based on Australian life tables and Redwood et al. [28]. All costs are reported in 2024 Australian dollars (A$). All future costs and QALYs are discounted at 5% per annum in line with national guidelines [23], with the discount rate varied in the sensitivity analysis. As Australia does not have an official cost-effectiveness threshold, we tested a range of cost-effectiveness thresholds in our analyses. Economic evaluation methods are described in detail in Appendix F and the analysis is conducted and reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 [29].
2.6 Sensitivity AnalysesWe performed deterministic—one-way and two-way—and probabilistic sensitivity analyses to explore the impact of uncertainty in key model parameters, including immunisation efficacy, potential bias in the ascertainment of hospitalisations and other clinical endpoints, immunisation product costs and healthcare resource costs and changes in the discount rate. We detail the parameter ranges and distributions explored in these analyses in Appendix I in the supplementary materials.
2.7 Software UsedThe transmission and clinical pathways models were written in Python, utilising the Polars dataframe library. The cost-effectiveness model was written in R (version 4.3.3) and the economic analysis was primarily performed using Tidyverse package. The package details and code are available at https://gitlab.unimelb.edu.au/julian.carlin/infant-rsv-modelling.
Comments (0)