
Remember me

A model previously described by Shah et al. was used to estimate and compare the PHI and CE of implementing a US meningococcal immunization intervention strategy versus a comparator strategy in adolescents [28].
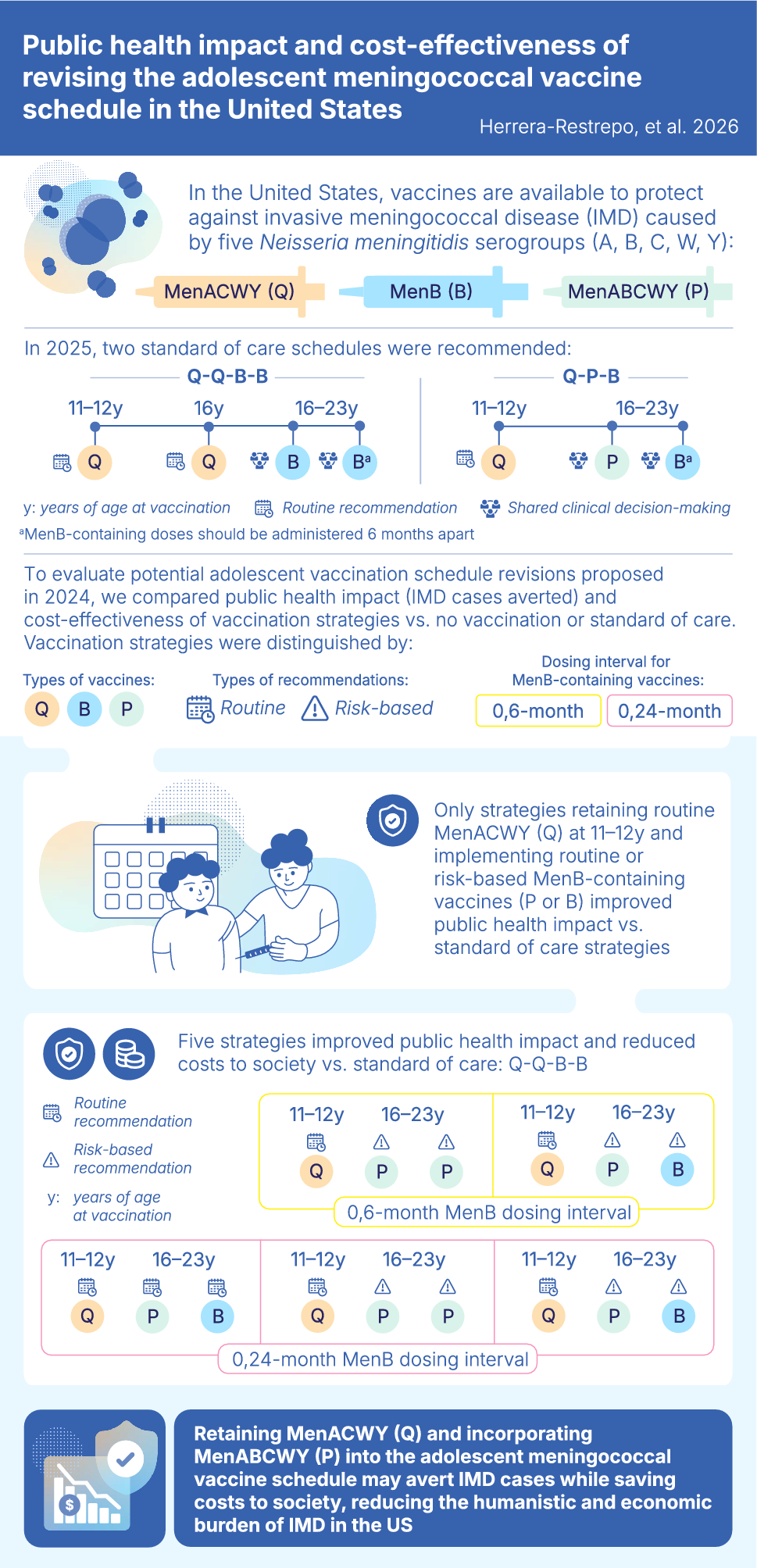
2.1 Schedule OptionsIn 2025, recommendations for vaccines to protect against IMD caused by serogroups A, B, C, W, and Y in US adolescents consisted of two schedules: (1) routine quadrivalent MenACWY (Q) at ages 11 and 16 years, monovalent MenB (B) under SCDM at ages 16–23 years, and B 6 months later (Q-Q-B-B); or (2) routine Q at ages 11 and 16 years, pentavalent MenABCWY (P) under SCDM at age 16–23 years, and B 6 months later (Q-P-B). These were considered standard of care in the model as they represented the CDC recommendations at the time of the study [12, 13].
The ACIP proposed five alternative meningococcal vaccine schedule options in June 2024, defined in terms of the number of serogroup-protecting vaccine doses to be administered, and reflecting differential vaccine recommendation types (i.e., routine, risk-based), ages at vaccine administration, and dose intervals for MenB-containing vaccine series (Table 1) [12].
Table 1 Adolescent meningococcal vaccine schedule options proposed by the ACIP in June 2024The five schedule options proposed by the ACIP informed the 27 unique vaccination strategies evaluated within the model (Table 2). Within each schedule option, multiple strategies were considered, varying on the basis of the type of vaccine (e.g., use of P in place of Q and B), type of recommendation (routine, risk-based), and dosing interval for MenB-containing vaccines (0,24-month, 0,6-month). Relative to SoC, the schedule options proposed by the ACIP (and their corresponding strategies) incorporate higher population-level coverage for MenB-containing vaccines due to routine recommendations (schedule options 1, 4, and 5) or risk-based recommendations (schedule options 2 and 3) for MenB-containing vaccines. Vaccine strategies were also distinguished on the basis of expected coverage for each vaccine dose, which would, in turn, affect public health impact. The 0,24-month dose interval (all a–c scenarios) was included to capture the ACIP’s consideration that longer dose intervals may provide extended protection against MenB at older ages. Populations at a higher risk of IMD due to serogroup B (i.e., healthy adolescents eligible for a risk-based recommendation) were defined as adolescents planning to attend college or those in congregate living situations (e.g., foster care, boarding school, correctional facilities). These designations were based on proposed CDC/ACIP definitions [30]. Intervention strategies with a 0,6-month dose interval were evaluated in alignment with Food and Drug Administration (FDA) labeling and potential improved implementation feasibility with a shorter dose interval due to more frequent HCP visits and higher MenB coverage rates at younger ages [21, 31,32,33,34,35].
Table 2 Intervention strategies derived from the meningococcal vaccine schedule options proposed by the ACIP and evaluated in the modelThe 27 intervention strategies were evaluated against comparator strategies, including no vaccination (NV) and SoC (Q-Q-B-B and Q-P-B; Table 2). A funnel approach was used, with PHI evaluated for all 27 intervention strategies, but CE only evaluated for strategies that improved PHI versus the SoC.
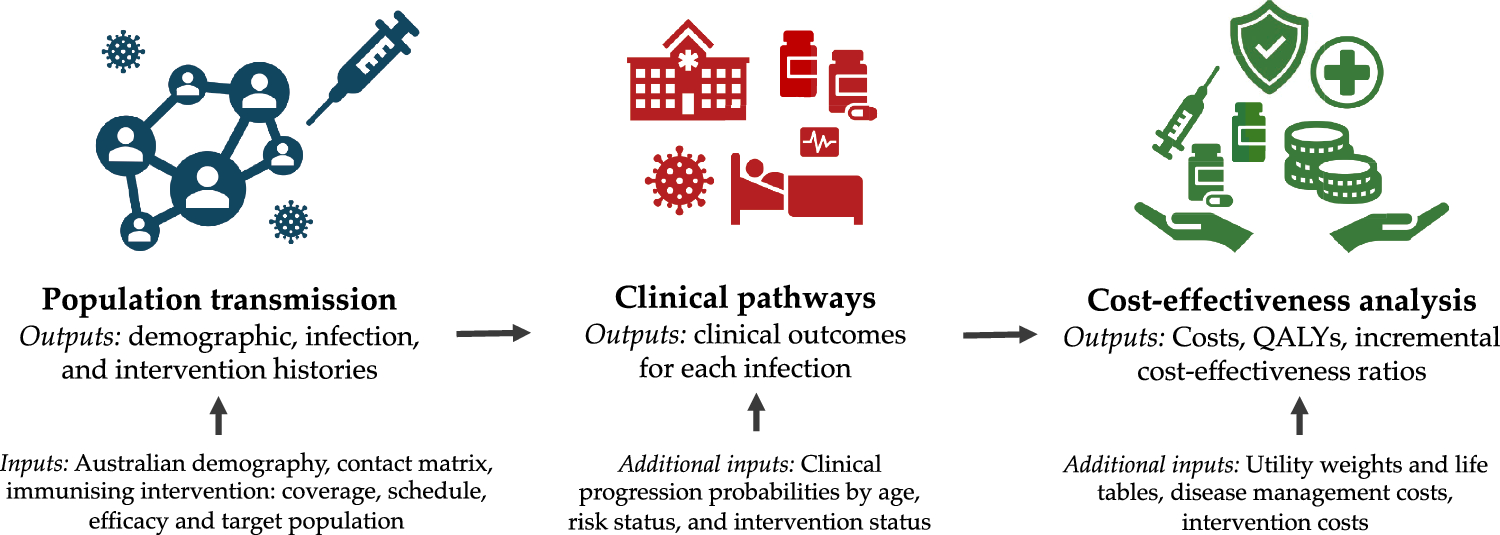
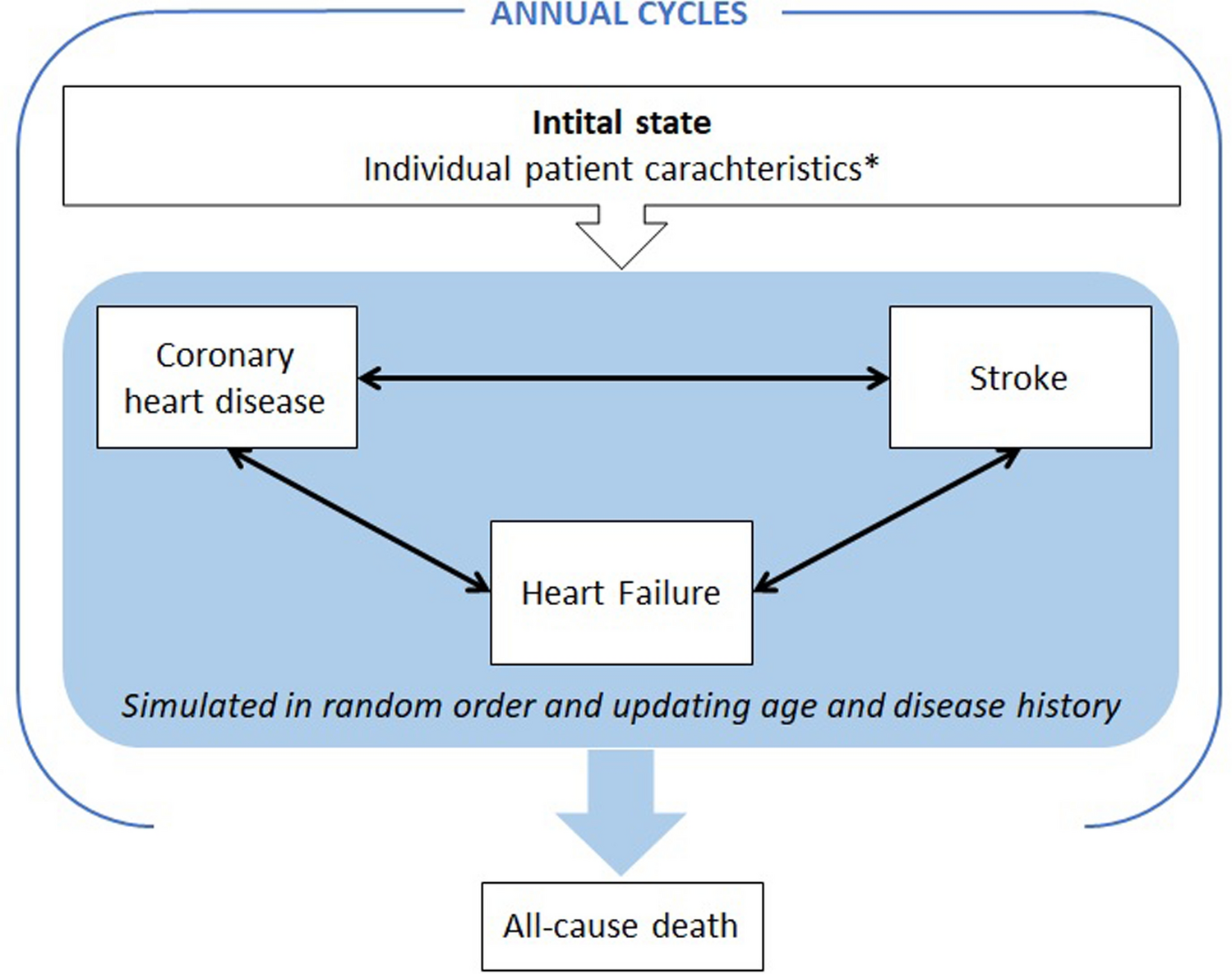
2.2 Model StructureThe model structure consisted of an epidemiological component to estimate IMD cases and an economic component to estimate the health and economic outcomes associated with IMD cases and vaccination costs incurred under the intervention and comparator strategies; a direct comparison of population-based health and economic outcomes between the intervention and comparator strategies was conducted. The model framework summarizing the CE and PHI analysis is presented in Fig. 1. The base case analysis evaluated the following outcomes of interest: IMD cases averted, IMD deaths averted, quality-adjusted life year (QALY) losses averted, incremental total societal costs, and incremental cost-effectiveness ratios (ICERs).
Fig. 1
Model structure. This figure summarizes the model framework to assess the PHI and CE of meningococcal vaccination intervention strategies. AEs included in the model represent serious AEs. AE adverse event, CE cost-effectiveness, IMD invasive meningococcal disease, PHI public health impact
2.2.1 Epidemiological ComponentThe epidemiological component estimated the IMD cases associated with each intervention strategy by utilizing population demographics, IMD incidence, vaccine coverage, and vaccine effectiveness data. Details of the methodology for the epidemiological component have been published previously by Shah et al. [28].
In summary, compartments segmented the population by protection status against MenB and MenACWY. Further, within each status, individuals were designated as those susceptible to carriage and those who were active carriers of each of three serogroup categories (B; A, C, W, and Y; and “other” pathogenic and non-pathogenic types; Supplementary Fig. 1).
When an individual received a vaccination, they moved from a compartment without protection to one with protection against a particular serogroup. The rate of transition between the unprotected and protected compartments was a function of vaccination coverage and efficacy as well as the number of individuals already protected against a particular IMD serogroup at the time of a transmission event. Not all vaccinated individuals acquired initial vaccination protection, however, and some that did initially acquire protection lost it due to waning. Acquisition of carriage resulted in transition from a susceptible compartment to a carriage compartment; upon recovery from carriage, those individuals transitioned back to a susceptible compartment. A portion of individuals who were carriers (and not protected against the serogroup they carried) developed IMD; carriers who were protected against the serogroup they carried did not develop IMD caused by that serogroup. Although transmission of meningococcal carriage was modeled dynamically, it was assumed that meningococcal carriage would be unaffected by vaccination against IMD caused by serogroup B or serogroups A, C, W, and Y, as there is limited evidence supporting carriage protection from meningococcal vaccination in the US. Given this paucity of evidence regarding carriage protection, carriage was assumed to be unaffected by vaccination and the model behaved similar to a static population-based model, with indirect effects (i.e., herd effects) of vaccination not captured. The decision to regard the model as static in nature served to avoid introducing uncertainties stemming from unknown vaccine effects on meningococcal carriage.
2.2.2 Economic ComponentThe economic component of the model was informed by the results of the epidemiological component as well as data concerning IMD health outcomes, IMD-related costs, and costs associated with vaccination.
The likelihood of death and sequelae per IMD case was calculated, as well as health and economic outcomes associated with each case. The 16 physical, psychological, and neurological IMD sequelae (Supplementary Table 1) were selected on the basis of the conclusions of a published panel of expert clinicians [8] and informed by available literature [2, 36,37,38]. Due to a lack of US-specific data on co-occurrence of sequelae, the incidence of each sequela was assumed to be independent of the incidence of other sequelae. Vaccination costs incurred under the intervention and comparator strategies were calculated as a function of vaccination coverage estimates and costs for acquisition, administration, and vaccine-related serious adverse events. Productivity losses related to receiving the vaccine were not included, as it was assumed that IMD vaccination would be administered as part of an existing preventive visit, thus additional productivity losses specific to IMD vaccination would not be incurred.
The base case analysis assumed a societal perspective, accounting for all costs incurred by the healthcare system (including all vaccination costs, direct costs for acute IMD care, and any direct costs associated with medical care for long-term sequelae), as well as special education and indirect costs (productivity losses for patients and caregivers) due to acute IMD and sequelae.
2.3 Model Overview2.3.1 PopulationThe modeled population consisted of the entire US population. Population estimates were stratified into 100 single-year age groups, between those aged 0–99 years, at the start of the model and modified on the basis of projected birth and all-cause death rates over time. Both meningococcal carriers and individuals considered to be protected against serogroups A, C, W, and Y due to vaccination prior to the start of the time horizon (2015) were included. Newborns entered the model at the beginning of each year on the basis of US birth projections, with mortality occurring at the end of each monthly model time step.
2.3.2 Time HorizonA 10-year initialization period began in 2015 (2015–2024) to reflect the period when both the MenACWY and MenB vaccines were available in the US, IMD incidence was relatively stable, and vaccination was assumed to be consistent with the SoC: Q-Q-B-B strategy. Following the initialization period, a 15-year evaluation period began in 2025, when the intervention and comparator strategies were assumed to begin; outcomes for the PHI and CE analyses were collected for the IMD cases occurring during 2025–2039 (15-year timespan). This evaluation time horizon was selected in alignment with the IMD CE assessments conducted by the CDC and GSK and presented during ACIP meetings in 2023 and 2024 [29, 39, 40]. Lifetime outcomes were collected for individuals with IMD, capturing the impact of IMD through direct and indirect long-term sequelae costs for each IMD case that occurred during the 15-year time horizon. Lifetime productivity loss costs due to premature death from IMD, as well as lifetime QALYs lost due to premature death from IMD or sequelae, were collected.
2.3.3 Discount RateAn annual discount rate of 3% was applied to all costs, life-years, and QALYs, including future costs and utility decrements resulting from long-term IMD sequelae (calculated on the basis of a patient’s remaining life expectancy) and costs and utilities incurred due to acute IMD (discounted on the basis of the year the IMD case occurred) [41]. The 2025 vaccine prices were used; all costs in the analysis were reported in 2025 US dollars, with cost inputs that were not originally reported in 2025 US dollars converted to that cost year using the medical care component of the US Consumer Price Index for direct medical costs and the General US Gross Domestic Product Price Deflator for indirect costs [42, 43].
2.4 Base Case InputsIMD incidence and case-fatality inputs were sourced from national surveillance data summarized in the CDC’s June 2023 ACIP meeting and published literature, respectively [37, 44]. Vaccine characteristics for each intervention strategy were sourced from the literature, clinical trial data, or on the basis of model assumptions. The epidemiological inputs utilized for the base case of this analysis were unchanged from those used to evaluate the PHI of IMD intervention strategy revisions, as detailed by Shah et al. [28], and are provided in Supplementary Table 1.
All cost inputs were obtained from published literature and national costing sources, including the Healthcare Cost and Utilization Project and Centers for Medicare and Medicaid Services (CMS) Physician Fee Schedule databases [45, 46]. Data regarding utilities, incidence, and costs associated with IMD sequelae were sourced from the published literature, expert clinical opinion, and/or assumptions (Supplementary Table 2).
Data on vaccine cost and coverage per intervention strategy were obtained from published literature and assumptions (Supplementary Table 3; Table 2), with MenABCWY inputs informed by the CDC’s analysis of the GSK MenABCWY vaccine [29, 47]. Vaccine prices were calculated using a weighted average of the actual public and private sector costs for each vaccine, the estimated market shares for each vaccine, and the percentage of vaccines purchased at the public and private sector costs. Vaccine administration costs were calculated using the weighted average of the actual public and private sector administration costs for each vaccine and the percentage of vaccines administered at the public and private sector costs. Market shares for each vaccine were assumed to be the same as in the 2024 CDC CE model for the GSK MenABCWY vaccine. As in the aforementioned CDC CE model, we assumed no vaccine wastage due to administration errors in our analysis [29, 47].
2.5 Base Case OutcomesEpidemiological outcomes included the annual number of IMD cases, IMD deaths, and occurrences of IMD sequelae by patient age and serogroup for each intervention or comparator strategy.
Economic outcomes included lifetime QALY losses for patients (due to acute IMD, IMD-related death, and long-term sequelae) and patients’ family and network (due to bereavement and care of patients with IMD in the acute phase and with long-term sequelae), with discounted life-years and QALYs also calculated to inform the economic component of the model. Costs included vaccination costs and total societal costs (i.e., costs associated with the health outcomes of each incident IMD case, including direct medical costs [acquisition, administration, and serious adverse events due to vaccination; IMD acute care costs; and costs due to IMD sequelae], direct nonmedical costs [special education costs], and indirect costs due to IMD [caregiving for patients with IMD by family and networks and market and nonmarket productivity losses for patients with IMD or their family members due to acute care, long-term sequelae, or premature death]).
Epidemiological and economic outcomes were then assessed across intervention and comparator strategies to determine PHI and CE. PHI outcomes of interest included cumulative IMD cases averted, IMD deaths averted, and QALY losses averted. The CE outcome of interest was the ICER of intervention versus comparator strategies, measured as incremental cost per QALY gained.
2.6 Analyses2.6.1 Base Case AnalysisAll base case results reflect cumulative outcomes for the entire US population in the years 2025–2039. The present analysis first explored intervention strategies that improved PHI versus SoC, then assessed associated costs, and finally, determined the CE of those strategies that improved PHI relative to SoC.
The PHI of each intervention strategy was calculated against NV and SoC options (SoC: Q-Q-B-B [routine MenACWY at ages 11 and 16 years and SCDM MenB at age 16 years and again 6 months later] and SoC: Q-P-B [routine MenACWY at age 11 years, SCDM MenABCWY at age 16 years, and SCDM MenB at age 16 years and 6 months]). The strategies that resulted in improved PHI versus SoC (i.e., more IMD cases averted, more deaths averted, and less QALYs lost) were subsequently evaluated to determine their total societal costs and total QALYs gained, and hence, their CE via ICERs.
2.6.2 Sensitivity AnalysesDeterministic sensitivity analyses (DSAs) were performed for schedule options that resulted in an improved PHI compared with SoC: Q-Q-B-B. DSAs were not performed versus SoC: Q-P-B due to uncertainties related to the recent introduction of pentavalent vaccines, which were addressed by scenario analyses. Only inputs for which ranges are specified were varied. All stratified inputs were varied together across stratifications (e.g., for inputs stratified by age, values applying to all ages were varied at once). The values were varied across reasonable ranges of upper and lower bounds while keeping all other parameters constant. Inputs with the largest impact on ICERs were sorted and arranged in descending order.
Probabilistic sensitivity analyses (PSAs) were also performed for schedule options that resulted in an improved PHI compared with SoC: Q-Q-B-B, to capture uncertainty in the estimates of incremental QALYs and incremental costs for intervention strategies versus the SoC. A Monte Carlo simulation with 500 iterations (found to be sufficient for the PSA to demonstrate convergence in the outcomes of interest) was used. Uncertainty in model parameters was assessed using probability distributions around corresponding base case values (Supplementary Table 2).
2.6.3 Scenario AnalysesGiven the lack of available data regarding real-world vaccine coverage of the SoC: Q-P-B recommendation [20], conversion from the MenB to MenABCWY vaccine in the base case economic analysis assumed full (100%) coverage conversion from MenB to MenABCWY for Q-P-B and Q-P-P intervention strategies. Coverage conversion was defined as the utilization of P in place of B, and full (100%) coverage conversion indicated that P vaccines fully replaced B vaccines (e.g., 75% conversion would indicate that P vaccines accounted for 75% of MenB-containing vaccine coverage, while B vaccines accounted for the remaining 25%). However, challenges due to the lack of interchangeability between MenB-component vaccines originating from different manufacturers and corresponding HCP concerns about potential maladministration, and HCP uncertainty regarding the use of the MenABCWY vaccine outside of the indicated FDA 2-dose vaccine series, can be noted as factors potentially leading to lower conversion rates from B to P in Q-P-B intervention strategies in real-world practice [48, 49]. Therefore, a scenario analysis exploring lower conversion rates was conducted among intervention strategies, which improved PHI in the base case scenario to assess the effect of these real-world implementation considerations. Conversions of 50% from B to P in Q-P-B and 75% from B to P in Q-P-P were assumed on the basis of the expectation that conversion to P would be higher in Q-P-P due to increased HCP willingness to use P in that vaccine schedule, compared with a schedule for which both P and B would need to be stocked (Q-P-B).
Comments (0)