2.1 Model Overview
The model considers the cost effectiveness of mRDTs as an adjunct to the SoC. SoC is defined as conventional culture and MALDI-ToF MS without mRDT. The analysis population consists of hospitalised adults suspected of BSI. The primary country setting is the United States (US), with the United Kingdom (UK) considered in a separate scenario. The perspective of the analysis is a US hospital. The primary outcomes are incremental costs and the quality-adjusted life years (QALYs) gained per patient. Additionally, the analysis estimates deaths averted and adverse events (C. difficile infection and AKI). A lifetime horizon is applied to the analysis in order to estimate QALYs gained. A 30-day time horizon is applied to costs and other intermediate outcomes in the model (e.g. C. difficile and AKI cases averted). Discounting was applied to QALYs at 3% per year following recommended guidance [22]. Costs were not discounted given the short time horizon for resource use (30 days).
The model was designed to capture the incremental benefit of each pathogen detected by mRDT following consideration of the clinical pathway for a patient admitted to hospital with a suspected BSI and the key points at which test results might influence outcomes (see Electronic Supplementary Material [ESM], Section 1.1). Guidelines recommend that patients with a suspected BSI be rapidly started on broad-spectrum antimicrobial therapy [23, 24]. Once the pathogen is identified, treatment may be optimised to a narrow-spectrum therapy targeting the particular pathogen. Optimising treatment to an effective targeted therapy is essential if the broad-spectrum therapy is ineffective. However, patients may benefit from a reduction in adverse events following optimisation (de-escalation) even if the broad-spectrum therapy is effective. In tandem with pathogen identification, the susceptibility of the pathogen to different antimicrobials is investigated. The results of the AST may identify resistance that renders the current therapy ineffective or susceptibility to a more preferred agent.
Current SoC, MALDI-ToF MS from plate cultured colonies, may typically require 16–24 h (post Gram stain) to generate pathogen ID results. This information must be communicated to the treating clinical team member to allow for potential optimisation of therapy. Typically, this is accompanied by guidance on optimisation of therapy provided by a specialist team as part of an antimicrobial stewardship programme (ASP).
When considering a molecular diagnostic approach, data on pathogens provided by mRDT differ in the level of granularity. We distinguished three levels of granularity: genus (such as all Enterobacter), group (such as K. pneumonia and K. quasipneumoniae but not other Klebsiella), and species. Data on species provides complete information on the species of the pathogen. Data on genus provides the genus or family to which the pathogen belongs. Data from group identify a group of different species of pathogen belonging to a particular genus. The model considers ID and subsequent actions on results at the species, group or genus level to be equivalent in the base case. In scenario analysis, the benefit of early ID is limited to species and group calls, or species calls only.
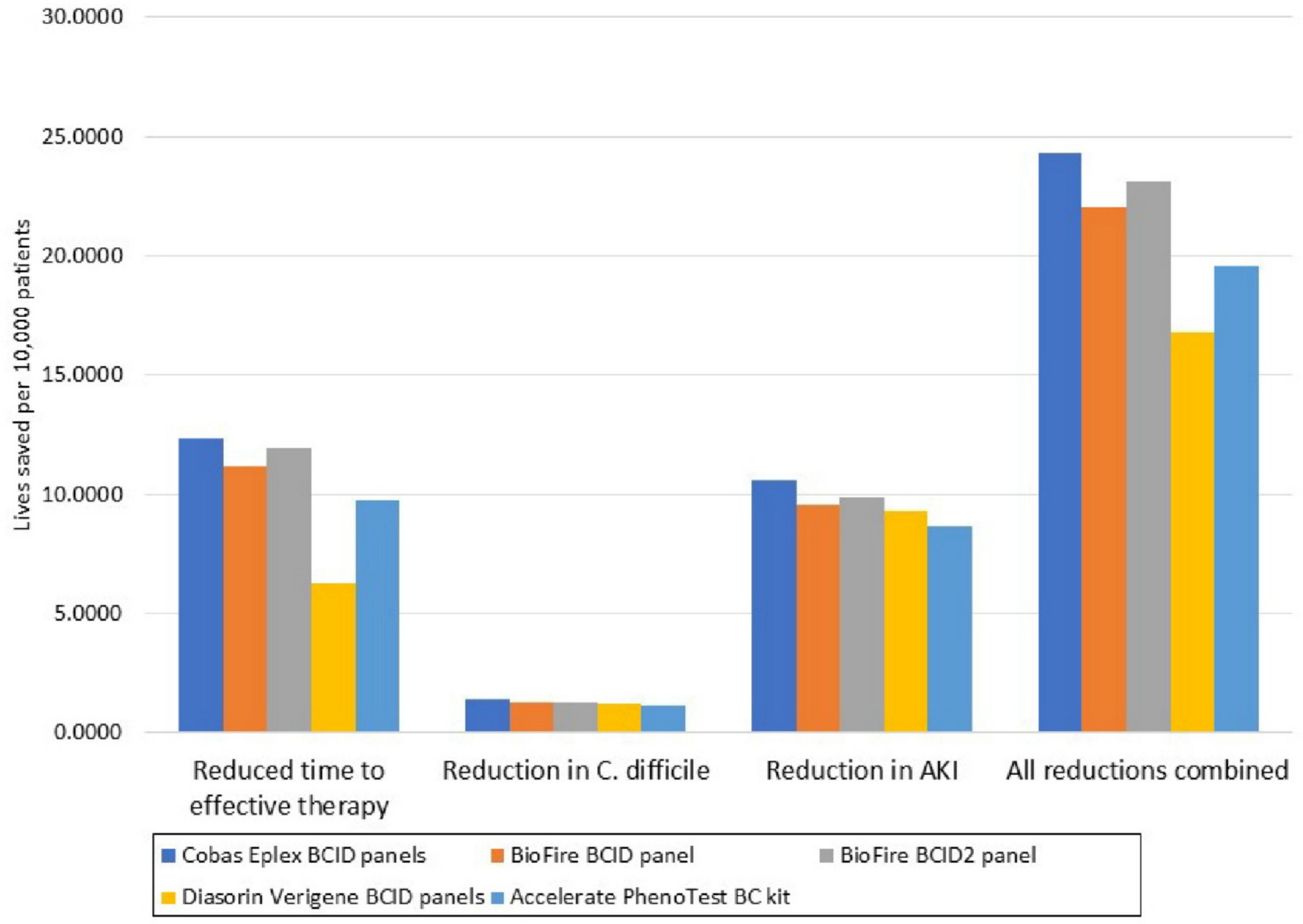
The model was structured to estimate the impact on mortality and LOS of reduction in the time to ID of the pathogen and of resistance mechanisms. Detection of pathogen with mRDT allows earlier optimisation of therapy. The model considers three adverse outcomes arising from non-optimal treatment: increased mortality arising from a delay to effective treatment, risk of C. difficile infection, and risk of AKI arising from extended exposure to broad-spectrum antimicrobial therapy. The model considers the proportion of patients receiving effective empiric antimicrobial treatment according to the causative pathogen. Where empiric antimicrobial treatment is ineffective, patients are subject to a delay to effective treatment which increases the risk of mortality and extended hospital stay. After ID of the pathogen (and resistance pattern), patients receiving effective empiric antimicrobial treatment or unnecessary antimicrobial therapy may be de-escalated to a targeted therapy (or no therapy in the case of a contaminant). These patients are at heightened risk of C. difficile infection and AKI while on broad-spectrum antimicrobial therapy.
The model captures mortality, adverse events and costs over the index period of hospitalisation (assumed to be up to 30 days). Survivors of the index hospitalisation are assumed to be subject to increased mortality for 5 years, following which they recover completely to their previous health status (assumed to be age/sex matched to the general population). Quality-adjusted life expectancy (QALE) of survivors is calculated assuming population data for mortality and health-related quality of life (HRQoL). Patient HRQoL during hospitalisation is assumed to be unaffected by any reduction in time to ID of pathogens or resistance mechanisms. Where a patient has a BSI with a resistance mechanism, changes to antimicrobial therapy are assumed to occur only after confirmation of the resistance mechanism. The key assumptions underpinning the analysis are described in Table 1.
Table 1 Main assumptions underpinning the analysis2.2 Intervention and Comparators
The SoC for detection of BSIs is set to be conventional culture plus MALDI-ToF MS without mRDT. Conventional antimicrobial susceptibility testing was assumed to be undertaken using phenotypic AST methods such as disk diffusion, broth microdilution and automated AST systems such as VITEK® 2, BD Phoenix™, or MicroScan®. Conventional MALDI-ToF MS typically requires longer culturation and hence physicians are assumed to receive the results of MALDI-ToF MS and to act on them 24 h post-Gram stain. The local hospital antibiogram provides an expected or empirical susceptibility pattern for pathogens identified by MALDI-ToF MS, but actual susceptibility must still be confirmed through AST that takes a further 24 h. Consequently, physicians are assumed to receive the required information to optimise therapy 48 h following Gram stain in the case of pathogens with intrinsic or typically well-known resistance patterns (like Pseudomonas aeruginosa).
The interventions considered in the analysis are summarised in Table 2. All relevant panels (Gram-positive, Gram-negative and fungal) were included for each mRDT. Results of mRDT are assumed to be provided to clinicians within 3 h after Gram stain, and clinicians to act on those results. Results of resistance mechanisms are assumed to be sufficient to allow selection of an effective targeted therapy. Hence, inclusion of an mRDT is assumed to reduce time to pathogen identification by 21 h and 45 h for non-resistant and resistant pathogens, respectively.
Table 2 Standard of care and interventions2.3 Model Parameters
A number of relevant parameters were sourced from a recent publication examining the relationship between receipt of appropriate antimicrobial therapy and mortality in 32,100 patients with a BSI across 183 US hospitals [32]. The study reported the proportion of patients for whom empiric antimicrobial therapy was effective across 17 broad species of pathogen. The effectiveness of empiric antimicrobial therapy ranged from 64.6% for Acinetobacter baumannii to 98.2% for Staphylococcus aureus. These data were used to determine the likelihood that empiric therapy is effective for each species of pathogen included in the analysis. The study also provided data on the relative proportion of Gram-positive, Gram-negative and fungal infections (46.59%, 52.50%, and 0.91%, respectively). An age of 65 years and a proportion of 45% women was assumed for the modelled cohort to align with the demographic data reported in the study. Finally, the study provided data on the number and class of antimicrobial therapies received by patients according to the type of BSI that was subsequently determined. Further details on the methods and data analysis are reported in the ESM, Sects. 2 and 3.
The model considered 82 common BSI pathogens (27 Gram-negative, 37 Gram-positive, 15 fungal, and 3 generic categories for the remaining species within each pathogen type). Data on the distribution of pathogen species within the three types were derived from data collected during the development of the Cobas Eplex BCID panels. The pathogen species and genera detected by each mRDT were determined from the product information for each of the panels [33,34,35,36,37] (ESM, Section 3.1.3). Pathogen species considered to be contaminants were guided by the literature [41] (ESM, Section 3.2.2). The base case assumed no mortality associated with pathogens categorised as contaminants. However, in scenario analysis, all species were assumed invasive. The base-case proportion of patients de-escalated from effective broad-spectrum antimicrobial therapy to a targeted therapy following ID of the pathogen or resistance mechanism was 62.9%, based on data at 72 h for a tertiary care medical centre in the US [42].
Data on mortality were taken from a recent Canadian study that included 19,326 patients. The study reported 30-day mortality for 29 pathogen species [43]. Mortality ranged from 12.1% for E. coli to 41.9% for Clostridium species. These data were used to estimate mortality under SoC for each of the 82 pathogens in the model under the assumption that deaths from BSIs occur in the first 30-day period. The data are reported in detail in the ESM, Section 3.1.6. Mortality after 30 days was taken from national life tables after applying a hazard ratio of 2.43 to the risk of death in the first 5 years. The hazard ratio was taken from a Finnish study comparing mortality over 5 years following cardiac surgery in patients with a BSI and in patients not tested for a BSI, and after excluding the first 30 days [44].
The impact of delays in receipt of effective therapy on mortality were taken from a recent Swedish study which reported odds ratios (OR) for mortality as a function of the delay to effective therapy based on analysis of 10,628 episodes of BSIs in adults [45]. A linear regression of the reported data estimated an increase in the OR of death of 0.01 for each hour of delay. Details of the analysis are provided in the ESM, Section 3.1.7. The data were used to calculate the reduction in mortality associated with a reduction in time to ID of the pathogen or resistance mechanisms, where an mRDT was able to detect the pathogen and empiric therapy is ineffective.
The LOS associated with a BSI was taken from a US publication reporting LOS for 830 patients with a BSI according to whether empiric antimicrobial therapy was effective or not [46]. Digitisation of Kaplan-Meier (KM) data provided a restricted mean LOS of 11.56 days for patients receiving effective broad-spectrum empiric therapy. The impact of delay to effective therapy on LOS was parameterised using data from a US study which reported the impact of delay to Gram stain notification on LOS [47]. A duration ratio of 1.004 (95% confidence interval [CI] 1.001–1.008) was reported for each hour of delay. This ratio was used to increase LOS from the base value of 11.56 days for every hour of delay to ID of the pathogen or resistance mechanisms for patients whose empiric therapy is ineffective.
The risk of C. difficile infection was taken from a US study reporting the incidence of C. difficile infection as a function of the sum of defined daily doses of antibiotics received by the patient [48]. The defined daily dose is a dose considered sufficient for one day of treatment according to the World Health Organization (WHO), and hence the sum captures the cumulative impact of multiple antibiotic treatments. The study reported crude risks of C. difficile infection of 1.32% and 3.01% for defined daily doses in the range 3.0 to 7.79 and 7.8 to 21.0, respectively. Linear interpolation between the two data points generated an absolute risk of 0.19% of C. difficile for each defined daily dose of antibiotic. Mortality from C. difficile infections of 8.6% was taken from a study reporting mortality from C. difficile infection in patients with sepsis [49]. An increase in LOS of 3.66 days was assumed following a C. difficile infection [50]. The source was a systematic review which pooled estimates according to the rigour of the methodology in the respective studies; the chosen value was reported for studies using time-varying matching techniques.
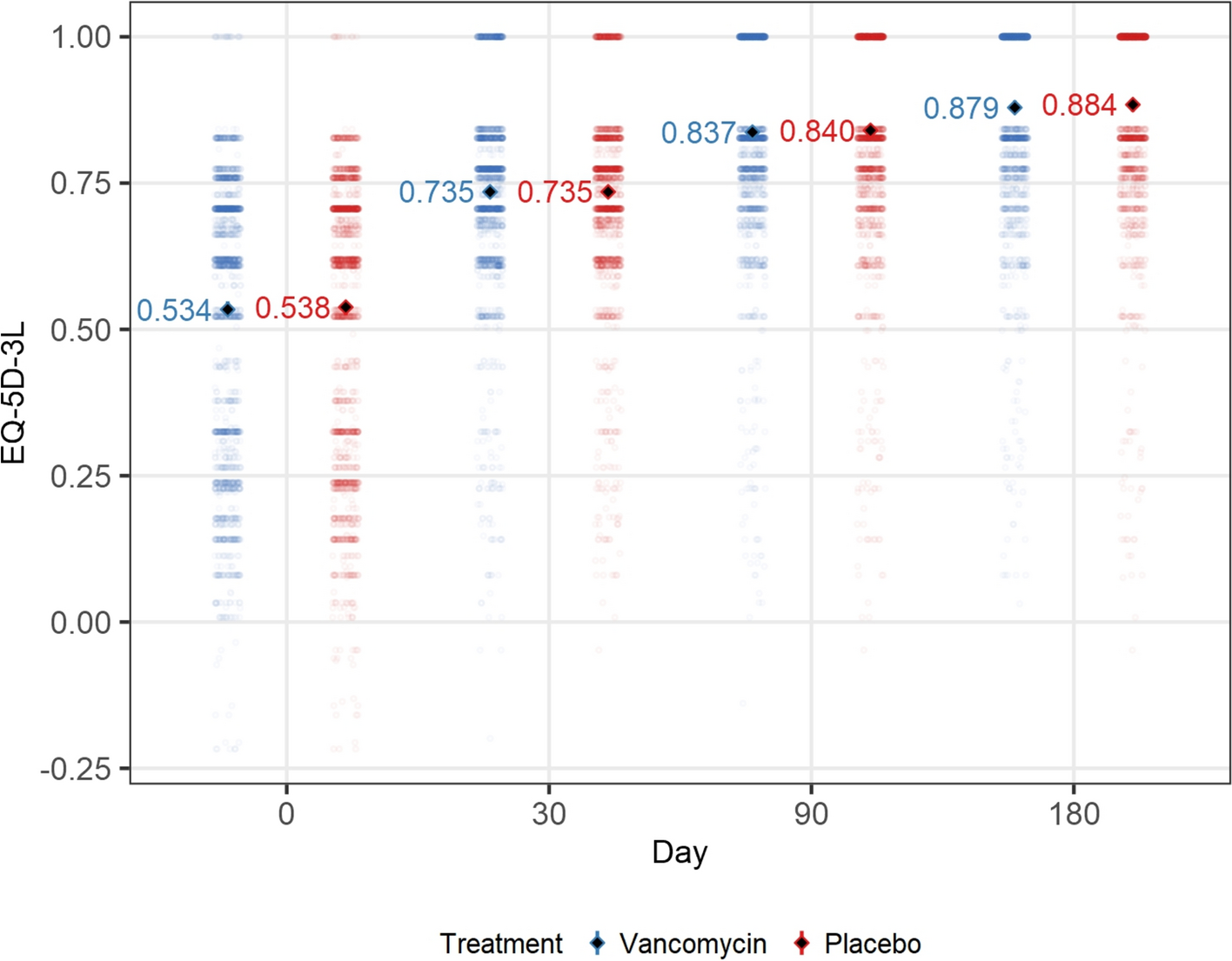
The risk of AKI was taken from a US study in patients receiving vancomycin at doses of ≥ 4 g/day and < 4 g/day, and patients receiving linezolid [51]. Data on time to nephrotoxicity for patients receiving < 4 g/day of vancomycin indicated a cumulative risk of 16.7% at 12 days. Assuming that the risk of AKI is constant over time, this equates to a daily risk of 1.51%. The model assumed a reduction in risk of AKI of 1.51% for every 24-hour reduction in the duration of broad-spectrum antimicrobial therapy. The impact of AKI on mortality was taken from a recent US study examining the incidence and outcome of AKI in patients with carbapenem-resistant Gram-negative infections [52]. Adjusted mortality was 18.5% in the group who experienced AKI (n = 91) compared with 5.6% in the group who did not (n = 659). The absolute difference of 12.9% was assumed as the mortality attributable to AKI. The impact of AKI on LOS was taken from a US study examining the incidence and severity of AKI associated with antimicrobial therapy [53]. The study reported median and interquartile range (IQR) for LOS in patients not experiencing and experiencing AKI of 11 (IQR 8–17) and 15 (IQR 11–23), respectively. The median LOS were converted to mean LOS of 11.53 and 15.84 days using the method of Wan et al. [54]. The difference between the mean values of 4.31 days was assumed to be the increase in LOS associated with AKI.
Data on the classes of empiric therapy received by patients (varying by class of pathogen) were taken from Ohnuma et al [32]. Expert clinical opinion was sought to identify the most likely antimicrobial regimen used for each of the classes of antimicrobial, and for the most likely targeted therapy for each pathogen species in the model. Data on dosing were primarily obtained from the British National Formulary [55] and combined with unit costs from the US Veteran Affairs drug pricing database [56] to allow estimation of the costs of broad-spectrum and targeted antimicrobial therapies (ESM, Section 3.2.2). The data allowed estimation of the cost impact of moving from broad-spectrum to targeted therapy.
Base-case costs were derived from a synthesis of market analysis data—incorporating public tenders, third-party market intelligence, and field-based intelligence—to estimate bundled ‘reagent rental’ prices. To account for the uncertainty in mRDT costs, threshold analysis was undertaken for the cost of each mRDT. The costs include reagents, rental and maintenance of the machine for a typical mid-sized hospital. The cost of MALDI-ToF MS did not impact the analysis since mRDTs were assumed to be used in addition to SoC (culture and MALDI-ToF MS). A cost of US$7.52 per sample, which included reagents and capital costs, was estimated based on data reported by Tran et al. [57] (ESM, Section 3.2.1). A cost of hospital stay per inpatient day of US$3025 was taken from data by the Kaiser Family Foundation (KFF) [58]. This is an all-inclusive cost of inpatient expenses including the cost of antimicrobials. Costs are reported in 2024 US Dollars (USD).
Key model parameters are summarised in Table 3.
Table 3 Key model parametersLife years accrued for survivors were estimated using US national life tables for 2020 [59]. Life years were discounted at 3%. Life years were weighted for HRQoL using utility data as a function of age and sex for the US population to estimate QALYs [60].
2.4 Analysis in a UK Setting
Scenario analysis was conducted to examine cost effectiveness in a UK setting. The scenario applied a National Health Service (NHS) perspective and outcomes were discounted at 3.5% following recommended guidance [22]. In this scenario, the distribution of pathogens, LOS in hospital, and unit costs were estimated from sources relevant to the UK. Data on test costs were not available in a UK setting and hence costs were estimated based on US prices. The GBP: USD exchange rate for 2024 was 1 USD: 0.782 GBP [61]. The purchasing power parity rate (PPP) for 2024 for health services was 1 USD: 0.679 GBP [62]. The analysis conservatively applied a rate of 1 USD: 1 GBP, and also applied the PPP rate. Utility data used to weight life years in order to calculate QALYs were also taken from a UK source [63]. UK data sources are detailed in the ESM, Sect. 3.2.
2.5 Sensitivity Analysis
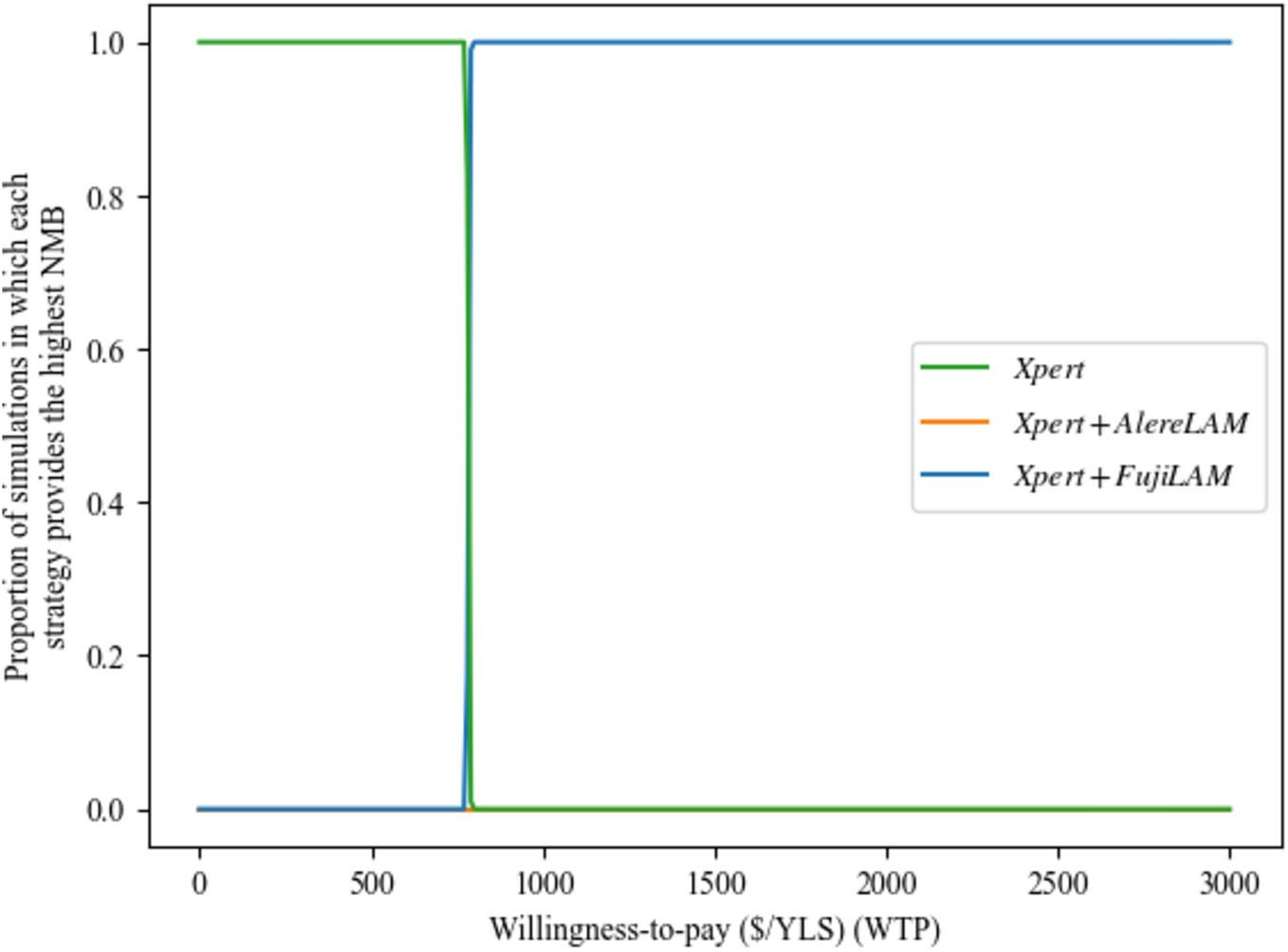
Probabilistic sensitivity analysis (PSA) was undertaken to quantify the impact of uncertainty across model parameters that were subject to sampling uncertainty. Distributions were assigned to each parameter reflecting natural bounds on plausible parameter values with standard errors estimated from the original parameter source, where possible, or assumed to be ±20% of the mean value. One thousand simulations of the model were run with each parameter value sampled from the specified distribution in each simulation. Results are reported as the cost-effectiveness acceptability curve.
One-way sensitivity analysis (OWSA) was performed on all parameters subject to sampling uncertainty (with the exception of life-table data and data on HRQoL as a function of age), with CIs informed by standard errors, where these data were available, or estimated as ± 20% of the point estimate. Threshold analysis was run on the cost of each mRDT to determine the cost at which each mRDT became cost effective at a threshold of US$50,000 per QALY.
The following scenario analyses were undertaken: exclusion of genus calls (treated as not identifying the pathogen); exclusion of genus and group calls; exclusion of contaminants (all pathogens assumed to be true infections rather than contaminants); reduction in the proportion of patients de-escalated from effective antimicrobial therapy to targeted therapy following pathogen or resistance ID; sensitivity of all mRDT assumed to be 95% for all pathogens detected; and application of a reduction in HRQoL of 0.12 for 5 years for BSI survivors.


Comments (0)