Study cohort and groups
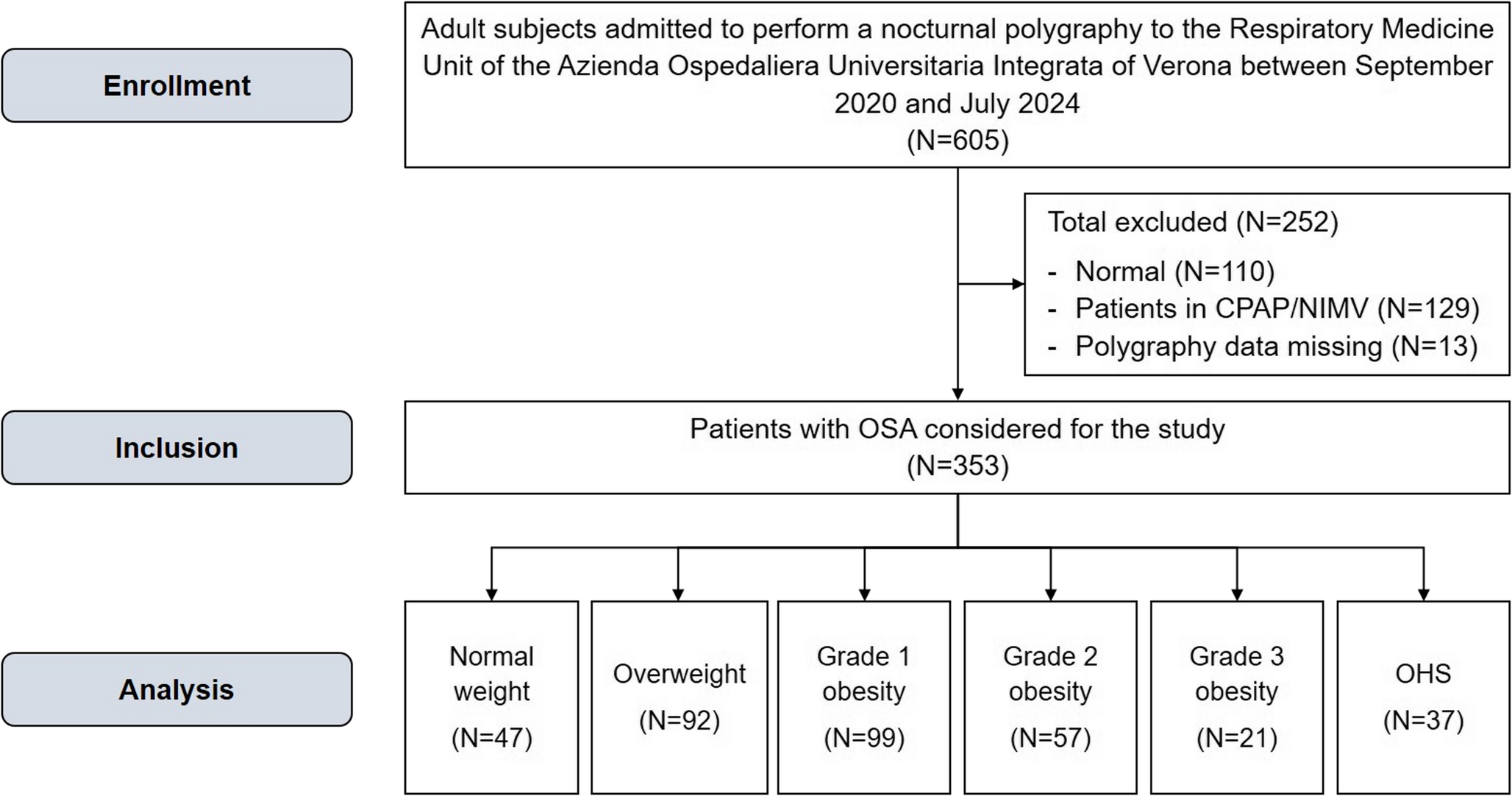
Between September 2020 and July 2024, we prospectively evaluated subjects referred for a suspected nocturnal respiratory disorder to the dedicated outpatient clinic of the Respiratory Medicine Unit at the Azienda Ospedaliera Universitaria Integrata of Verona. We excluded: (1) subjects with normal polygraphy; (2) patients with OSA or OHS receiving any form treatment; (3) patients with causes of nocturnal hypoventilation other than OHS [20]; and (4) patients with missing or of poor quality respiratory polygraphy data.
Based on body weight, patients with OSA were categorised as normal weight (BMI 18.5–24.9 kg/m2), overweight (BMI 25.0–29.9 kg/m2), grade 1 obesity (BMI 30.0–34.9 kg/m2), grade 2 obesity (BMI 35.0–39.9 kg/m2), grade 3 obesity (BMI ≥ 40.0) [21, 22], and OHS [7].
The study protocol was approved by the hospital ethics committee and conducted in accordance with Good Clinical Practices guidelines and the Declaration of Helsinki.
General measures
Demographic and anthropometric characteristics, including neck, waist, and hip circumferences, prevalence of arterial hypertension, heart disease, diabetes, and peripheral arterial disease (PAD), as well as lifestyle information (smoking habits and pack-years), were collected.
Nocturnal polygraphy and daytime sleepiness
Respiratory polygraphy was performed using a portable Nox T3s™ device (https://noxmedical.com, USA). Only recordings with adequate signal quality were included. The following signals were acquired: peripheral oxygen saturation (SpO2) measured by a finger sensor, thoracic and abdominal movements assessed by inductive belts, nasal airflow derived from the belts, snoring, and body position. This portable device has demonstrated excellent measurement agreement with to in-lab polysomnography [23]. The device’s signals were analysed using the Noxturnal™ software, with an advanced automated respiratory scoring algorithm. Each recording was subsequently reviewed by a pulmonologist with expertise in sleep medicine, who confirmed respiratory events and the final scoring. According to the American Academy of Sleep Medicine International Classification of Sleep Disorders, third edition [24], respiratory polygraphy includes total sleep time (TST) and the apnoea-hypopnoea index (AHI), calculated as the number of apnoeas and hypopnoeas per hour of sleep (n/h). Apnoea was defined as the absence of airflow for ≥ 10 s, while a hypopnoea was defined as a ≥ 30% reduction in airflow associated with an oxygen desaturation ≥ 3%. AHI severity was classified as mild (AHI ≥ 5 and ≤ 15 events/h), moderate (AHI > 15 and ≤ 30 events/h), and severe (AHI > 30 events/h) [1]. OHS was defined according to established criteria [7].
Pulse oximetry parameters included lowest SpO2, oxygen desaturation index (ODI, defined as the number of events per hour of oxygen desaturation of 3% ODI), mean desaturation depth, and sleep time with SpO2 < 90% (ST90) [1].
Daytime sleepiness was assessed using the Italian version of the ESS [25], an eight-items self-reported questionnaire evaluating the likelihood of falling asleep in daily situations.Total scores range from 0 to 24 [12, 25], with ESS > 10 indicating excessive DS [12].
Statistical analysis
The assumption of normality was assessed using the preliminary Kolmogorov-Smirnov test. Categorical variables are reported as number and percentage, and continuous variables as median with interquartile range (IQR). Group comparisons were performed using χ2 or Fisher’s exact tests for categorical variables and nonparametric Mann-Whitney U or Kruskal-Wallis H tests for continuous variables.
Associations between variables were evaluated using the Spearman’s correlation coefficient (ρ).
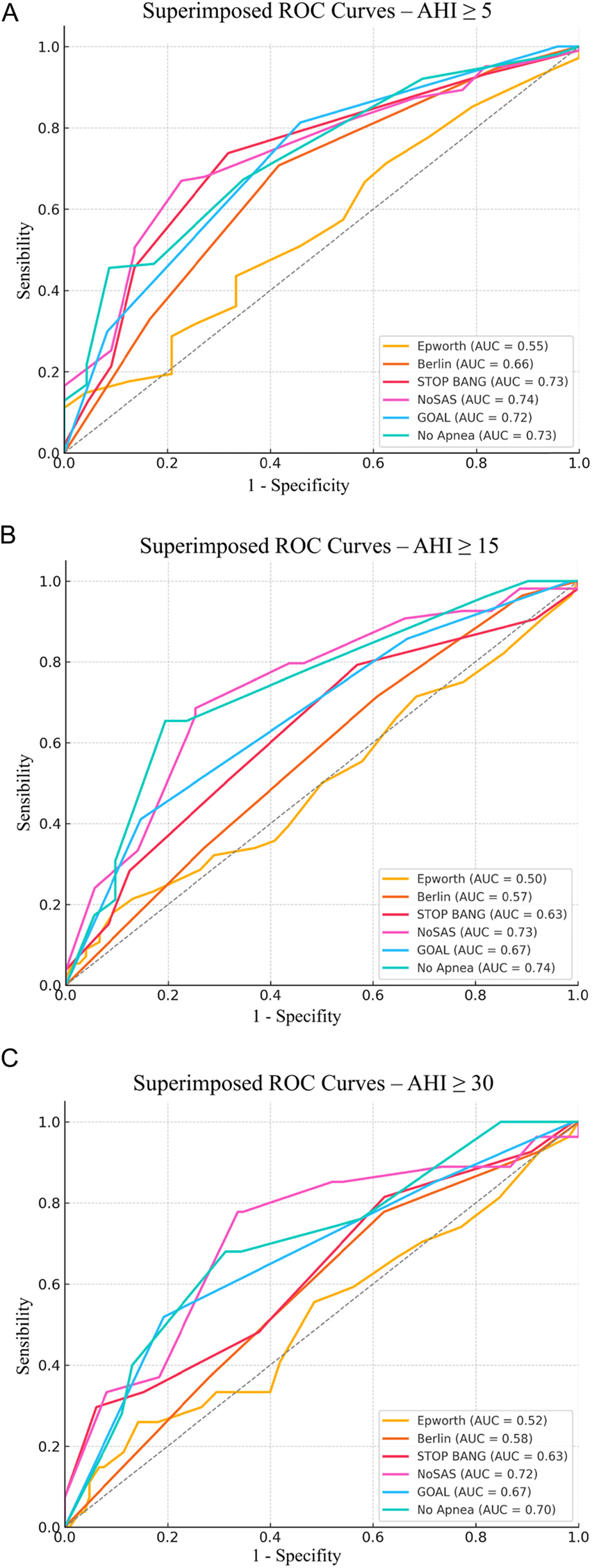
Univariate and multivariate mixed models were used to identify factors associated with excessive sleepiness perception (dependent variable: ESS > 10) [12]. The following variables were included in the analysis: age, sex, obesity grade (reference: normal weight), smoking status, neck, waist, and hip circumferences, arterial hypertension, heart disease, diabetes, PAD, AHI severity, ODI, lowest SpO2, mean desaturation, and ST90. Collinearity was assessed using Spearman correlations, and variables with strong correlations (r > |±0.50|) were excluded from multivariate models. Multicollinearity was evalated using the variance inflation factor (VIF). Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated [26]. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test [27]. Receiver operating characteristic (ROC) analysis and area under the curve (AUC) were used to identify the cut-off values for continuous variables significantly associated with excessive DS in multivariate models (means desaturation).
All analyses were performed using IBM SPSS, version 17.0 (IBM Corp., Armonk, NY, USA), and p-value < 0.05 were considered statistically significant.

Comments (0)