This study investigated the prevalence and characteristics of SDB in a monocenter cohort with more than 200 patients with HFpEF. As a result, SDB using an AHI cut-off ≥ 15/h was a frequent comorbidity in patients with HFpEF with a higher prevalence of OSA compared to CSA. Importantly, patients with CSA differed from patients with OSA significantly with regard to clinical characteristics, comorbidities, NT-proBNP levels and echocardiographic findings. Patients with CSA had more advanced heart failure as indicated by a higher HFA-PEFF score, a higher NYHA heart failure class and higher NT-proBNP levels, whereas patients with OSA had a higher BMI and a higher ESS score indicating increased daytime sleepiness.
Previous studies investigating SDB in HFpEF
The results of 11 previous studies reporting the prevalence of SDB in patients with HFpEF are summarized in Table 4. The reported prevalence of SDB in these studies varied considerably between 36% in the large German SchlaHF-XT multicentre study reported by Arzt et al.[11] and 83% in the study by Kishan et al.[9]. This wide range of SDB prevalence in HFpEF patients in previous studies may in part be explained by several important differences between these studies. Only three previous studies [2, 6, 8] enrolling small numbers of HFpEF patients used gold standard polysomnography, whereas all other studies [3,4,5, 7, 9,10,11,12] including our present study used polygraphic devices, which can underestimate the extent of SDB and particularly CSA. Furthermore, 5 previous studies [3, 7, 9,10,11] excluded patients with a history of SDB from study enrollment, whereas the remaining 6 studies [2, 4,5,6, 8, 10] did not exclude patients with known SDB. Finally, previous studies used different methods to diagnose HFpEF as well as various scoring rules for OSA and CSA. Importantly, previous studies used different AHI cut-offs as summarized in Table 4. When using AHI cut-offs defining respiratory events, one has to keep in mind that AHI has shortcomings since AHI primarily captures the number of apneas and hypopneas while ignoring the lengths of apneas and other important forms of SDB, such as flow limitation or respiratory effort-related arousals or disruptions in sleep without meeting the thresholds for apneas or hypopneas.
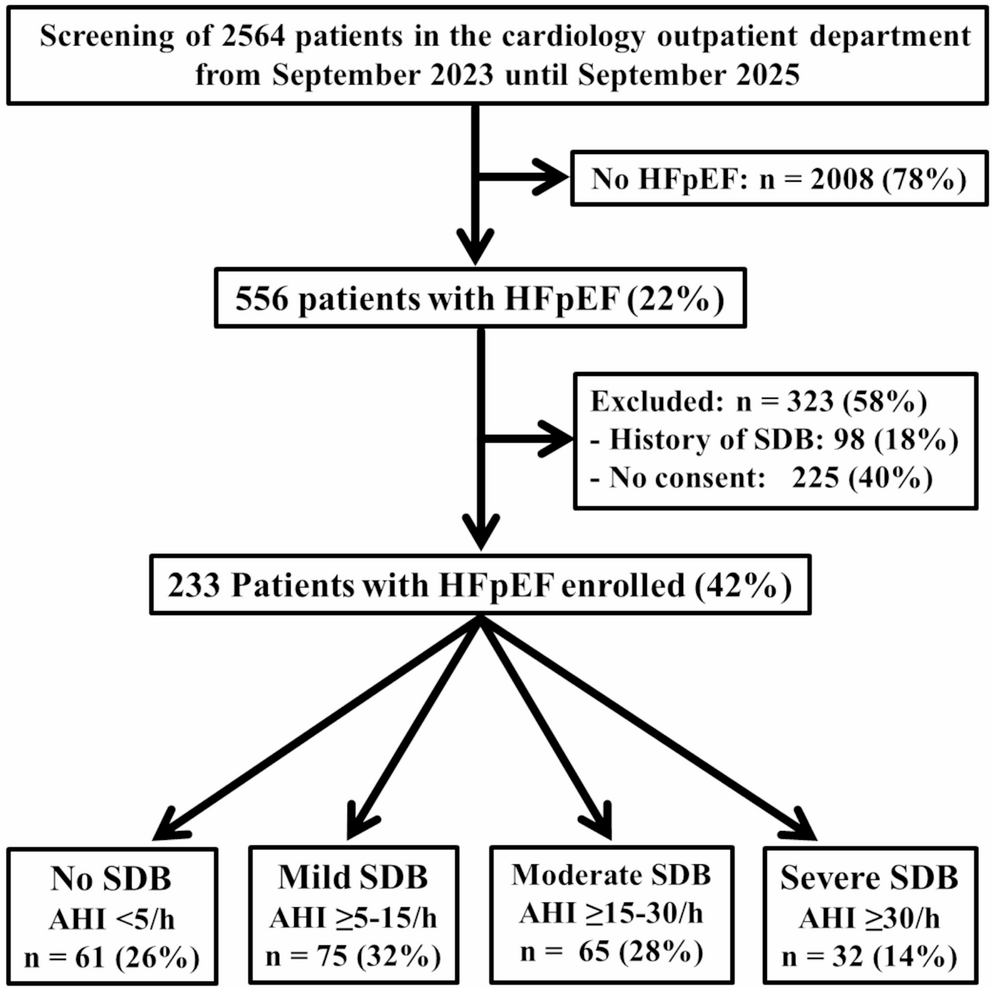
Table 4 Previous studies investigating the prevalence of SDB in patients with HFpEFUsing the same AHI cut-off ≥ 15/h to define moderate to severe SDB as Arzt and coworkers [11], we found a 42% prevalence of SDB in HFpEF, which is only slightly higher than the prevalence of 36% reported by Arzt and colleagues [11]. When using an AHI cut-off ≥ 5/h to define SDB in our study, the prevalence of SDB in our study rises to 74%, which is comparable to the SDB prevalence of 79% reported by Borrelli et al.[7] and the prevalence of 80% reported by Herrscher et al.[4] who used an AHI cut-off ≥ 5/h to define SDB in HFpEF. If Borrelli et al.[7] had used an AHI cut-off ≥ 15/h to define SDB, the prevalence of SDB decreased to 44% (Table 4).
The prevalence of 14% for CSA in HFpEF patients in our study does not confirm the high prevalence of CSA in HFpEF of 29% reported by Bitter et al.[3] and 38% reported by Borrelli et al.[7] or the low prevalence of CSA in HFpEF of 7% in the SchlaHF-XT study by Arzt et al.[11]. The discrepancies between these studies may in part be explained by differences in patient populations as well as various scoring rules for OSA and CSA. The prevalence of 14% for CSA in our study is comparable to the results reported by Herrscher et al.[4], Gupta et al.[8], Huang et al.[10] and Wang et al.[12], who reported a CSA prevalence ranging from 12% to 18% (Table 4).
In contrast to our present study, Arzt et al.[11] and Wang et al.[12] also investigated the prevalence of SDB in patients with heart failure with reduced left ventricular ejection fraction (HFrEF) in addition to HFpEF. Both investigators found a significantly higher prevalence of CSA in HFrEF compared to HFpEF suggesting an inverse relationship between CSA prevalence and LV ejection fraction. This finding is consistent with the results of a previous study at our institution in patients with HFrEF [23], in which we found a 43% prevalence of CSA using an AHI cut-off ≥ 15/h in patients with HFrEF versus 14% in patients with HFpEF in our present study.
Predictors of SDB in patients with HFpEF
By univariate comparison of patients with and without SDB, several previous studies reported a significant association between SDB and male gender [7, 9, 11], NT-proBNP or BNP levels [6, 7], body mass index [7, 9, 11, 12], NYHA heart failure class [11], older age [11], and various parameters for the degree of diastolic dysfunction [2, 3, 8] in patients with HFpEF. Comparability of these findings, however, is limited by several factors. Most previous studies did not evaluate potential important predictors of SDB simultaneously and only 4 previous studies [7, 9,10,11] used multivariate analyses. In addition, several previous studies did not report NT-proBNP or BNP values [2, 9, 11] as recommended by current heart failure guidelines of the European Society of Cardiology [13, 14], while other studies did not report any parameters of echocardiographic diastolic dysfunction for patients with SDB compared to patients without SDB2, [4, 8,9,10].
Similar to our study, Bitter et al.[3] found significantly higher NT-proBNP values in patients with CSA but not in patients with OSA compared to patients without SDB suggesting that patients with HFpEF and CSA have more severe heart failure than patients with HFpEF and OSA or patients with HFpEF without SDB.
Similarly, Borrelli et al.[7] described significantly higher NT-proBNP levels and age as predictors of nocturnal CSA, whereas BMI and arterial hypertension predicted OSA during nighttime. Using multivariate analysis, Borrelli et al.[7] found no predictor for CSA at nighttime, whereas we could demonstrate that the HFA-PEFF score [21], which is exclusively based on natriuretic peptide levels and echocardiographic measurements of diastolic dysfunction and age are predictors of CSA in patients with HFpEF by multivariate analysis. In contrast to patients with CSA, multivariate analysis revealed a significant association between OSA and male gender, BMI and LV mass index but not NT-proBNP levels in our study.
Despite several design similarities between our study and previous studies [2,3,4,5,6,7,8,9,10,11,12], our study has important strengths compared to previous studies. First, the most important comorbidities of HFpEF, NT-proBNP levels, renal function as well as comprehensive echocardiographic evaluation of diastolic dysfunction [15] were determined prospectively in all study patients as recommended by current heart failure guidelines of the European Society of Cardiology [13, 14]. Secondly, we enrolled 233 patients with HFpEF, whereas only 3 of 12 previous studies [3, 10, 11] listed in Table 4 enrolled more than 200 patients with the largest patient cohort being reported by Arzt et al.[11] in the SchlaHF-XT study. Our study is, however, to our best knowledge, the first study which calculated both H2FPEF and HFA-PEFF scores in all patients as recommended by current heart failure guidelines of the European Society of Cardiology [13, 14, 21].
Study limitations
Since many patients with HFpEF were enrolled during their first visit at our cardiology outpatient department, only approximately half of the patients were treated with sGLT2-inhibitors, which have been shown to improve prognosis in HFpEF and have received a class I indication for HFpEF therapy in current heart failure guidelines [3, 14]. To address this limitation, adjustment for all patients’ medications listed in Table 1 as potential confounding factors was performed during multivariate analysis. Another limitation is the use of cardiorespiratory polygraphy rather than gold standard polysomnography to detect SDB. Polygraphy can underestimate CSA, especially hypopnea-related central events. Furthermore, CSA in our study was defined based on predominance of central apneas, rather than the proportion of all central respiratory events including hypopneas. Finally, the number of patients with CSA in our study was modest, which limits statistical power for multivariate analysis and residual confounding remains possible, particularly from unmeasured factors.

Comments (0)