
Remember me
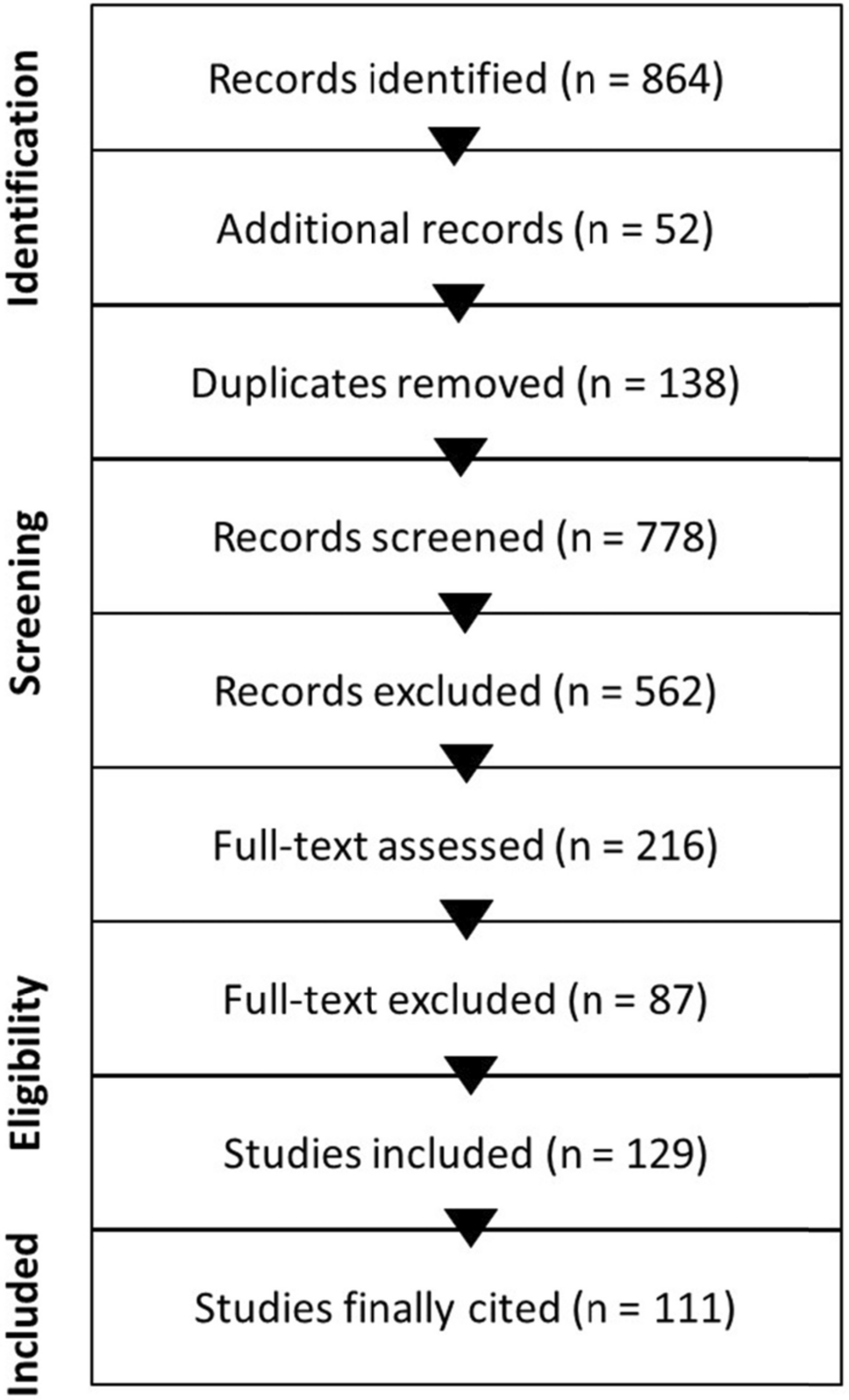
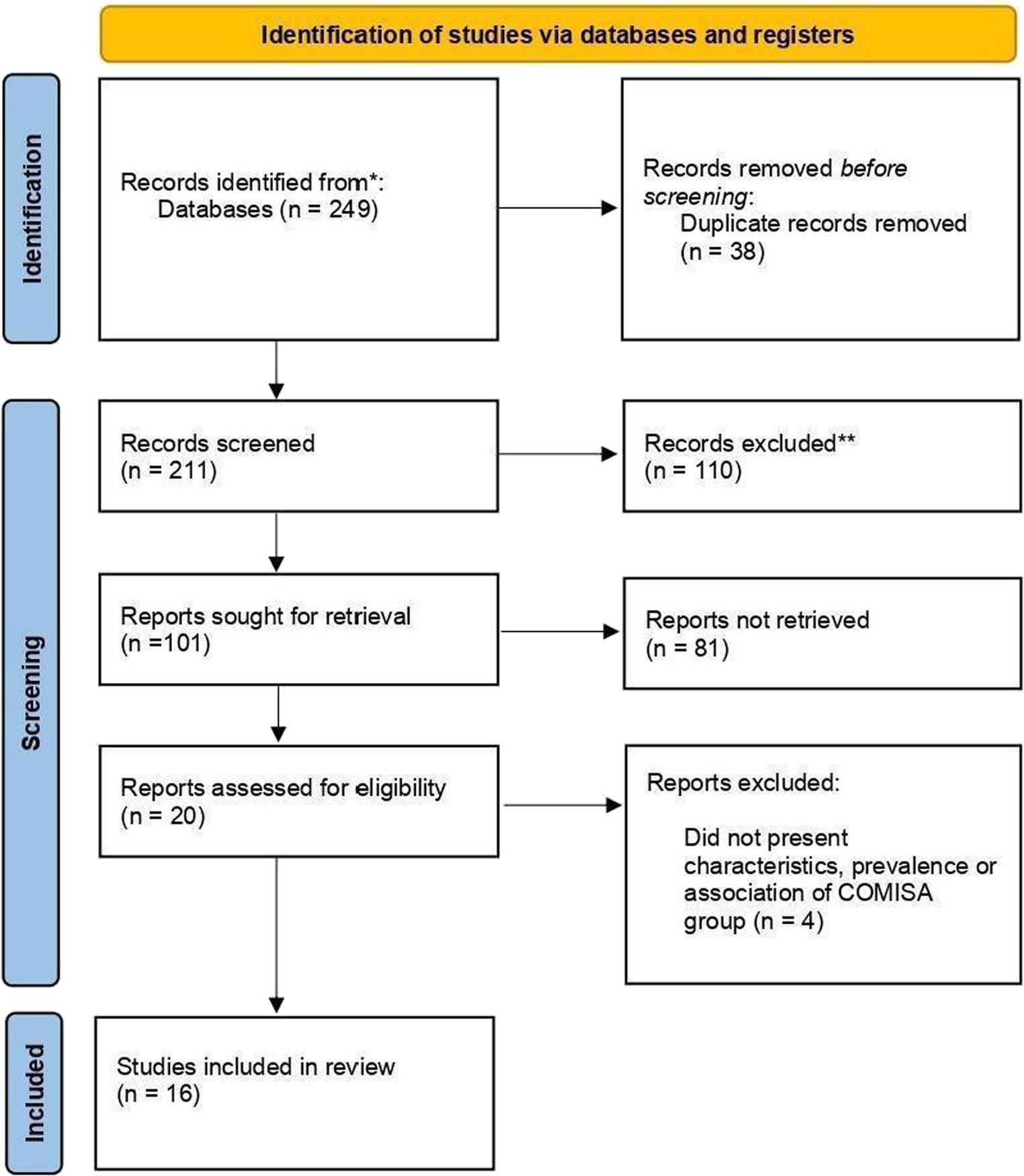
Initially, 249 records were identified in the databases. Thirty-eight duplicates were excluded, leaving 211 for the next phase. During the title screening, 110 records were excluded, and 81 were excluded during the abstract screening for not meeting the inclusion criteria, resulting in 20 studies. After full-text review, 4 studies were excluded, leaving 16 studies for the systematic review and meta-analysis. No records were found through manual search.
Therefore, 16 studies were selected for qualitative data synthesis, as shown in Fig. 1 and Supplementary Material 1.
Fig. 1
Flow diagram (PRISMA, 2020)
Examining the study characteristics, the selected studies included more than 9,700 participants across a total of sixteen observational studies. The mean age of participants was 42.56 years. Based on five studies [16,17,18,19,20] that reported sample size (N), mean BMI, and Standard Deviation (SD), the combined weighted mean BMI was approximately 30.79 kg/m², with a combined standard deviation of approximately 6.79 kg/m². The studies were conducted in various countries, including Portugal, Brazil, the United States, Iran, India, China, Mexico, the Netherlands, Israel, Norway, South Korea, Iceland, and Australia, as shown in Supplementary Material 2.
The assessment of Obstructive Sleep Apnoea and Insomnia (COMISA), sleepiness, fatigue, mood disorders, depression, anxiety, sleep, breathing, and gray matter was performed using instruments based on the criteria of the International Classification of Sleep Disorders (ICSD-2/3) and/or DSM-IV, as shown in Supplementary Material 3.
Risk of bias analysisAs shown in Supplementary Material 4, eight studies were classified as having a low risk of bias and, consequently, high quality, while eight studies were evaluated as having a moderate risk of bias, indicating moderate quality. For cross-sectional studies, the items with lower ratings were mainly related to question 5 and question 6. In the case-control study, the items with lower ratings were question 1, question 2 and question 3.
Meta-analysisFor the construction of the meta-analysis, COMISA event frequencies were used to determine prevalence in the studied general population, age group, geographic region, and BMI. The random-effects model was applied to all data analyses due to the high heterogeneity among studies.
For the first analysis (COMISA prevalence), all 16 studies were included, and the results indicate a prevalence of 30% for COMISA in the studied population (95% Confidence Interval (CI): 0.19 to 0.44, p < 0.05; I² = 99%), as illustrated in Fig. 2.
Fig. 2
COMISA Prevalence among participants in the selected studies
For the age-group analysis, three subgroups were created: mean age above 40 years [9, 16, 18, 21,22,23,24,25,26,27,28], mean age between 18 and 40 years [17, 19], and children and adolescents [29]. The results indicate a COMISA prevalence of 33% in the population over 40 years (95% CI: 0.19 to 0.51, p < 0.05; I² = 99%), 39% in the population aged 18 to 40 years (95% CI: 0.30 to 0.49, p > 0.05; I² = 26%), and 12% in the population of children and adolescents (95% CI: 0.06 to 0.22, p < 0.05; I² = 89%), as shown in Figs. 3 and 4, and 5.
Fig. 3
Prevalence of COMISA among participants over 40 years
Fig. 4
Prevalence of COMISA among participants aged 18 to 40 years
Fig. 5
Prevalence of COMISA among children and adolescent participants
For the geographic region analysis, three subgroups were created: European countries [20,21,22, 28], Asian countries [16, 18, 23, 24, 27, 29], and American countries [9, 17, 19, 26]. The results indicate a COMISA prevalence of 42% in European countries (95% CI: 0.09 to 0.85, p < 0.05; I² = 99%); 31% in Asian countries (95% CI: 0.14 to 0.57, p < 0.05; I² = 99%); and 35% in American countries (95% CI: 0.19 to 0.55, p < 0.05; I² = 98%), as shown in Figs. 6 and 7, and 8.
Fig. 6
Prevalence of COMISA in European countries
Fig. 7
Prevalence of COMISA in Asian countries
Fig. 8
Prevalence of COMISA in American countries
An analysis of COMISA prevalence was conducted specifically for Brazil [2, 9] and the United States [17, 26]. The results indicate a prevalence of 37% for COMISA in the United States (95% CI: 0.15 to 0.67, p < 0.05; I² = 99%) and 20% in Brazil (95% CI: 0.18 to 0.22, p > 0.05; I² = 0%), as shown in Figs. 9 and 10.
Fig. 9
Prevalence of COMISA in the USA
Fig. 10
Prevalence of COMISA in Brazil
In the sex-based analysis, the results indicate a prevalence of 59% of COMISA in the male population (95% CI: 0.51–0.66, p < 0.05; I² = 87%), as shown in Fig. 11. In the analysis by Body Mass Index (BMI), the findings indicated an average BMI of 28.55 (± 1.12) among participants with COMISA (95% CI: 26.34 to 30.76; p < 0.05; I² = 98%), as illustrated in Fig. 12.
Fig. 11
Prevalence of COMISA in men
Fig. 12
For the meta-analysis involving polysomnograpy indicators, 09 studies were used [16, 17, 19, 21, 23, 24, 27,28,29]. To allow standardized comparative analysis, all variables originally described as Median (P25-P75) were converted to the format Mean (± estimated SD). The transformation was carried out based on the valid approximation for symmetric distributions, where: SD ≈ (P75 - P25)/1.35. This factor (1.35) represents the typical width of the interquartile range in a standard normal distribution, as shown in Supplementary Material 5.
The studies by Pan et al., 2024 [18], Subramanian et al., 2021 [26], Bjorvatn 2014 [22], Hilmisson 2019 [20], Luciano 2024 [9], and Lang (2017) [25] were excluded for not presenting results in accordance with the criteria established for this meta-analysis.
Figure 13 displays the studies that presented polysomnography indicators in patients with COMISA and isolated OSA. The results show that there is a small statistically significant difference between the COMISA and OSA groups, MD = −1.24 (95% CI: −2.19 to −0.29, p < 0.05, I² = 94%), which can also be observed in the following polysomnography indicators: AHI: MD = −7.28 (95% CI: −11.88 to −2.68, p < 0.05, I² = 88%); Arousal Index: MD = 2.74 (95% CI: 0.47 to 5.00, p < 0.05, I² = 45%), Sleep Efficiency: MD = −4.04 (95% CI: −4.73 to −3.35, p < 0.05, I² = 67%) and Sleep Latency: MD = 3.05 (95% CI: 0.63 to 5.47, p < 0.05, I² = 66%), except for SpO₂: MD = 0.62 (95% CI: −0.52 to 1.76, p > 0.05, I² = 0%); Microarousal Index: MD = −0.91 (95% CI: −2.13 to 0.30, p > 0.05, I² = 35%) and REM Sleep Duration: MD = −0.61 (95% CI: −1.44 to 0.22, p > 0.05, I² = 34%), which did not show statistically significant differences between the groups. For the Arousal Index and Sleep Latency, the higher means are on the COMISA group.
Fig. 13
Polysomnography Indicators in patients with COMISA and isolated Obstructive Sleep Apnoea (OSA)
Figure 14 shows the studies that presented polysomnography indicators in patients with COMISA and isolated insomnia. The results show that there is a small statistically significant difference between groups: MD = 2.52 (95% CI: 0.67 to 4.36, p < 0.05, I² = 99%), which can also be observed in the following polysomnography indicators: AHI: MD = 16.07 (95% CI: 8.56 to 23.57, p < 0.05, I² = 97%), Minimum SpO₂: MD = −5.79 (95% CI: −8.94 to −2.63, p < 0.05, I² = 83%), Microarousal Index: MD = 5.21 (95% CI: 1.20 to 9.23, p < 0.05, I² = 95%), except for Arousal Index: MD = 0.67 (95% CI: −5.65 to 6.98, p > 0.05, I² = 85%); Sleep Efficiency: MD = −1.99 (95% CI: −4.60 to 0.62, p > 0.05, I² = 69%); Sleep Latency: MD = −3.86 (95% CI: −9.13 to 1.41, p > 0.05, I² = 68%) and REM Sleep Duration: MD = 0.49 (95% CI: −0.89 to 1.87, p > 0.05, I² = 39%), which did not show statistically significant differences between the groups. For the polysomnography indicators AHI and Microarousal Index, the higher means are on the COMISA group.
Fig. 14
Polysomnography Indicators in patients with COMISA and isolated Insomnia
The grading of recommendations assessment, development and evaluation - GRADEThe strength of the evidence for the analysis conducted between COMISA and isolated Obstructive Sleep Apnoea was considered high for the polysomnography indicators AHI and Arousal Index. For the other indicators, it was considered Moderate, as shown in Supplementary Material 6.
The strength of the evidence for the analysis conducted between COMISA and isolated Insomnia was considered high for the polysomnography indicator AHI. For the Microarousal Index and REM Sleep Duration indicators, it was considered Moderate. As for the other indicators, it was considered low as shown in Supplementary Material 7.
Comments (0)