This study provides a combined subjective and objective evaluation of sleep in pediatric oncology patients compared with their healthy siblings, offering novel insights into sleep-disordered breathing (SDB), psychological distress, and the influence of hospitalization on sleep physiology [3, 4, 29, 30]. Several key findings emerged.
First, subjective sleep disturbances were highly prevalent among both patients and siblings, consistent with prior literature reporting elevated sleep disruption in families facing pediatric cancer [3, 29,30,31,32]. Although most children exceeded the CSHQ cut-off, the PSQI identified a substantially smaller proportion as “poor sleepers.” This discrepancy highlights the known limitations of the PSQI in pediatric and mixed samples, where its sensitivity can be reduced, and parent-reported tools such as the CSHQ may better capture sleep behaviors [6,7,8, 14, 16,17,18]. Together with previous work emphasizing measurement issues in subjective pediatric sleep assessment [6, 8], our findings underscore the importance of using pediatric-appropriate instruments in clinical research and practice.
Second, patients exhibited significantly higher trait anxiety levels than their healthy siblings. This aligns with previous studies demonstrating heightened psychological burden in children undergoing cancer treatment due to disease uncertainty, procedural stress, and treatment-related fatigue [33,34,35,36,37,38,39,40]. Interestingly, state anxiety levels were comparable between groups, suggesting that chronic, baseline anxiety rather than acute situational anxiety may be more strongly associated with sleep disruption in this population. This pattern is consistent with data showing persistent anxiety and stress-related symptoms among pediatric oncology patients and survivors, as well as discrepancies between child and parent reports of anxiety in chronic illness [33, 38,39,40].
Elevated trait anxiety may contribute to hyperarousal and increased sympathetic activity, which could partially explain the higher resting heart rates observed in the patient group [41,42,43].
Third, objective respiratory parameters revealed a consistent, clinically meaningful pattern: children with cancer demonstrated significantly higher AHI, RDI, and ODI values than their healthy siblings. These findings indicate an increased burden of SDB in oncology patients, which may be related to treatment effects, upper-airway changes, alterations in autonomic regulation, or disease-associated inflammation [11, 12, 29, 44]. Elevated overnight heart rates in the patient group further support increased sympathetic activation during sleep, a physiologic marker of sleep fragmentation and autonomic stress previously described in pediatric populations and in conditions characterized by heightened inflammatory and hypothalamic–pituitary–adrenal axis activation [41,42,43,44].
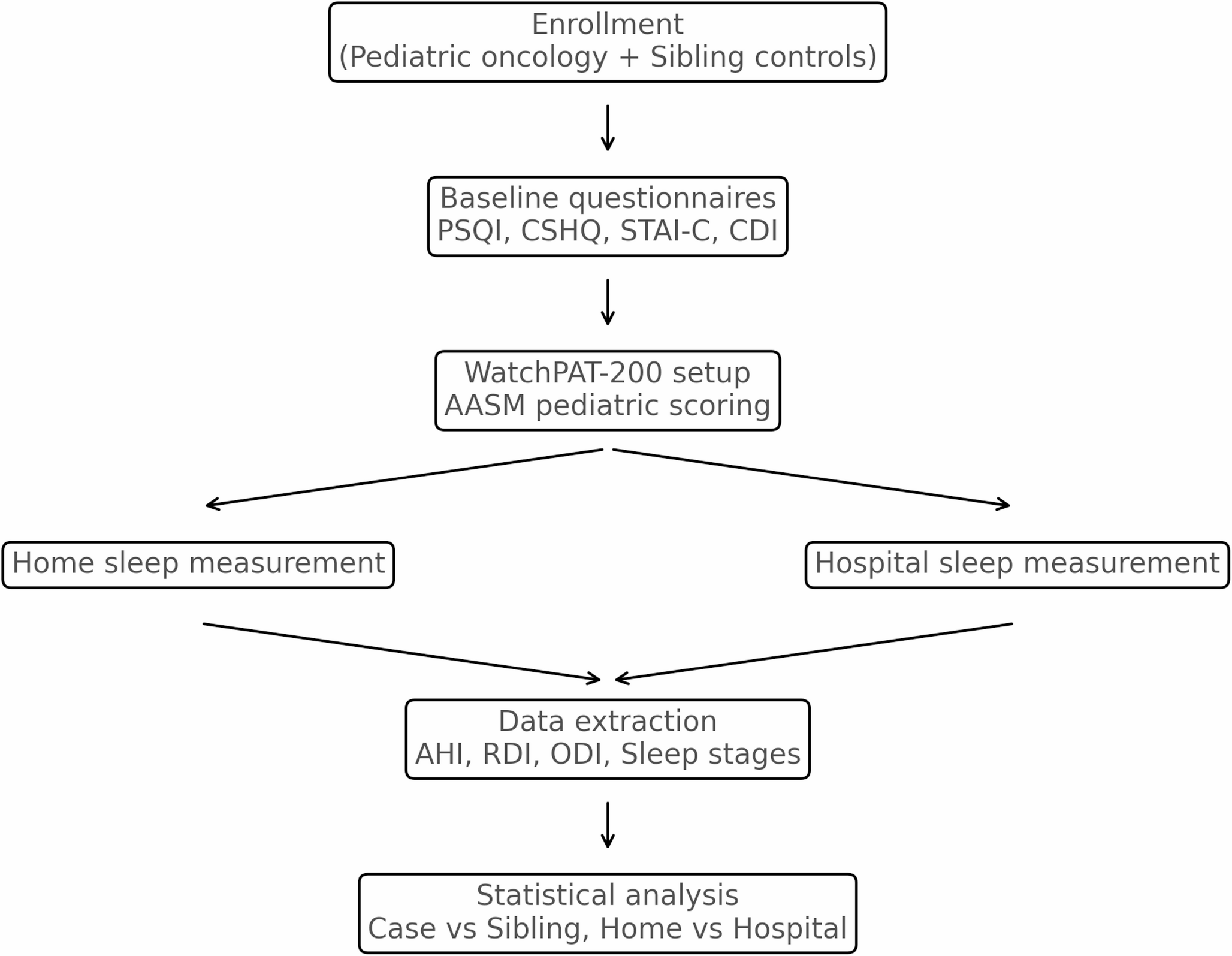
An essential contribution of this study is the comparison of home and hospital sleep recordings. Under conditions standardized to reduce nocturnal interruptions, there were no significant differences in respiratory parameters between environments. This suggests that the intrinsic effects of illness and treatment may outweigh environmental influences on sleep quality [3, 30]. Alternatively, the standardized hospital environment in our protocol may have mitigated typical inpatient sleep disruptions such as light, noise, or frequent staff awakenings [8, 30, 45]. These findings support the feasibility of using home-based devices in pediatric oncology, particularly when longitudinal monitoring is required.
Although WatchPAT provides valuable information on respiratory physiology, its use in children is constrained by developmental differences in autonomic regulation and by the absence of EEG-based sleep staging [23,24,25,26,27,28]. Therefore, the sleep-stage data reported here were interpreted cautiously and presented as exploratory outcomes. The primary analyses focused on SDB-related measures (AHI, RDI, ODI), which have stronger validation for PAT-based assessment and are increasingly used in pediatric and adult sleep research [25,26,27,28].
This study has several strengths, including the use of sibling controls, combined subjective and objective assessments, and dual-environment monitoring. Nonetheless, limitations should be acknowledged. The sample size was modest, which may limit statistical power for some comparisons and preclude detailed subgroup analyses. Cancer types and treatment regimens were heterogeneous, potentially introducing variability in sleep outcomes [3, 29]. WatchPAT, while practical and validated as a screening tool for SDB, does not replace gold-standard polysomnography and may underestimate certain events [23,24,25,26,27,28]. Finally, although environmental factors were standardized during hospital assessments, residual influences cannot be entirely excluded [8, 30, 45].
Overall, our findings emphasize that pediatric oncology patients experience clinically relevant sleep impairment and increased respiratory disturbances compared with their siblings. These results underscore the importance of incorporating routine sleep screening and objective sleep assessment into pediatric cancer care [3, 29,30,31,32, 46, 47]. Early identification of sleep problems may offer opportunities to reduce fatigue, improve psychological well-being, and enhance overall quality of life in this vulnerable population [5, 29, 31, 32, 44].
Clinical implications and recommendations
Therefore, it is crucial to include standard sleep assessments as part of the comprehensive care delivery for children with cancer. In other words, sleep disturbances are not just a secondary inconvenience; they can impair the immune system, worsen fatigue, and adversely affect emotional well-being [5, 29, 44]. Our findings support the safety and feasibility of a home-based sleep monitoring device in pediatric patients. The absence of significant differences between home and hospital settings underscores the device’s feasibility and the potential for its use in longitudinal or multicenter clinical protocols.
Addressing sleep disruption may provide opportunities to improve overall quality of life and treatment outcomes. To achieve a better approach for these patient groups, interventions could include behavioral treatments for insomnia (such as Cognitive Behavioral Therapy for Insomnia), environmental controls in hospitals (e.g., reducing light and noise), family sleep hygiene education, and drug treatments, following a sleep evaluation [48].
Strengths and limitations of the study
An important limitation of this study is the choice of subjective sleep assessment tools. Although the Children’s Sleep Habits Questionnaire (CSHQ) is a well-validated pediatric instrument, the Pittsburgh Sleep Quality Index (PSQI) was originally developed for adult populations and may be less sensitive in detecting sleep disturbances in children. Pediatric-specific instruments such as the Sleep Disturbance Scale for Children (SDSC), developed by Bruni et al., evaluate multiple domains of sleep disturbances and may provide a more comprehensive assessment in pediatric populations. Therefore, the use of PSQI in this study may have underestimated the prevalence or severity of subjective sleep problems [49].
The main strengths of this study include the simultaneous assessment of subjective sleep experiences, psychological factors, and objective respiratory parameters in both home and hospital settings using a sibling-controlled design. However, several limitations must be acknowledged. The sample size was relatively small, which may limit the statistical power of inevitable comparisons. Cancer types and treatment regimens were heterogeneous, potentially introducing variability in sleep outcomes. In addition, WatchPAT does not provide EEG-based sleep staging, may underestimate aspects of sleep quality, and lacks polysomnographic validation, limiting comparisons with gold-standard sleep metrics. Nonetheless, the stability of respiratory indices across environments suggests feasibility for use in multi-setting pediatric monitoring rather than definitive robustness. Finally, medication use—particularly corticosteroids—was not fully controlled and may have affected sleep physiology.

Comments (0)