Study design
We conducted a prospective, cross-sectional, descriptive, and analytical study to evaluate the diagnostic performance of several obstructive sleep apnea hypopnea syndrome (OSAHS) screening tools compared with respiratory polygraphy.
Study population and inclusion criteria
Patients were consecutively recruited from those referred to the Sleep and Home Respiratory Assistance Unit of the Centre Hospitalier Universitaire de Martinique, Department of Pulmonology, for suspected OSAHS between October 2023 and January 2025, until the required sample size was reached.
Inclusion criteria were:
Non-inclusion criteria were:
Sample size calculation
Assuming a type I error (α) of 5%, a power of 80%, a reference theoretical prevalence of 30–50%, and an expected prevalence of 70% (in this higher-risk referred population), the number of subjects required was estimated at 80 for score evaluation and 130 for association analyses. The sample size was increased by 20% to account for potential missing data. The final sample size (n = 134) met the a priori target for association analyses and exceeded the minimum required for questionnaire performance evaluation; however, the study was not powered for extensive subgroup or internal validation analyses.
Questionnaires
All included patients completed a paper questionnaire that collected their medical history, treatments, anthropometric measurements, and responses to six OSAHS screening tools: Epworth Sleepiness Scale, Berlin Questionnaire, STOP-BANG, NoSAS, GOAL, and No-Apnea.
Missing questionnaire items were retrieved from medical records if the patient had been hospitalized within the previous three months. When items remained missing after medical-record review, questionnaires with incomplete data were excluded from score calculation.
Respiratory polygraphy
All patients underwent overnight home-based respiratory polygraphy for a minimum of 6 h, including:
oxygen saturation monitoring by oximetry.
nasal–oral airflow recording.
snoring quantification using tracheal sound recordings.
respiratory effort measurement using thoracic and abdominal belts.
body position analysis.
All polygraphy recordings were manually reviewed and scored according to current international recommendations by experienced clinicians from the sleep unit. Recordings with insufficient duration or poor signal quality were excluded to limit misclassification.
Polysomnography was not available in our unit before May 2024 and has remained available only in limited capacity since then. Therefore, respiratory polygraphy was used as the reference standard for defining OSAHS cases. Before May 2024, patients requiring polysomnography were referred to other sleep laboratories, where waiting times often exceeded 12 months.
Exclusion criteria
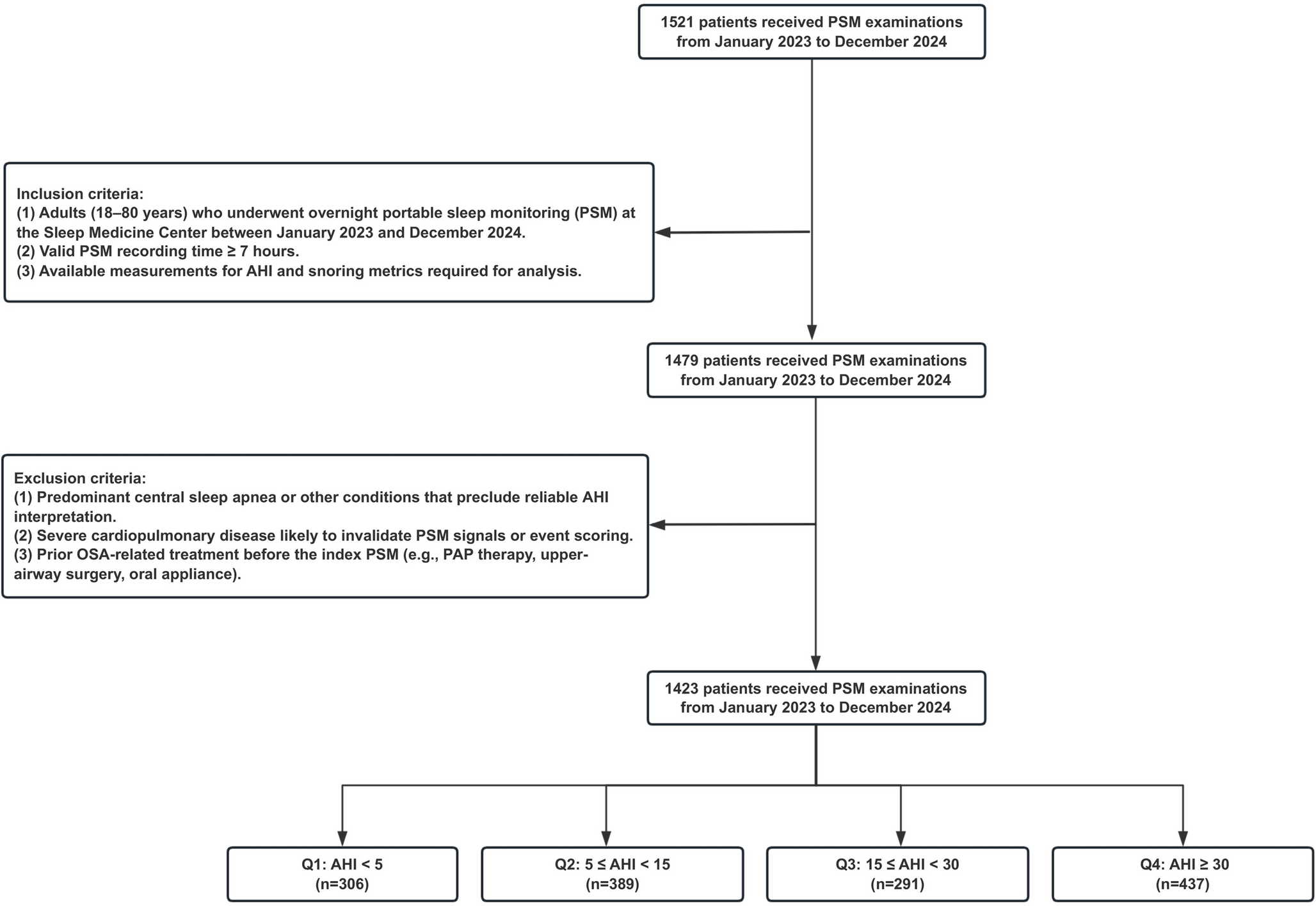
Patients who completed the questionnaires but did not undergo respiratory polygraphy (n = 13) and those with invalid polygraphy (insufficient recording time (n = 21), poor signal quality (n = 1), or missing data (n = 2) were excluded. A total of 134 patients remained out of the 171 initially included.
Statistical analysis
Data were entered in Microsoft Excel and analyzed using Python.
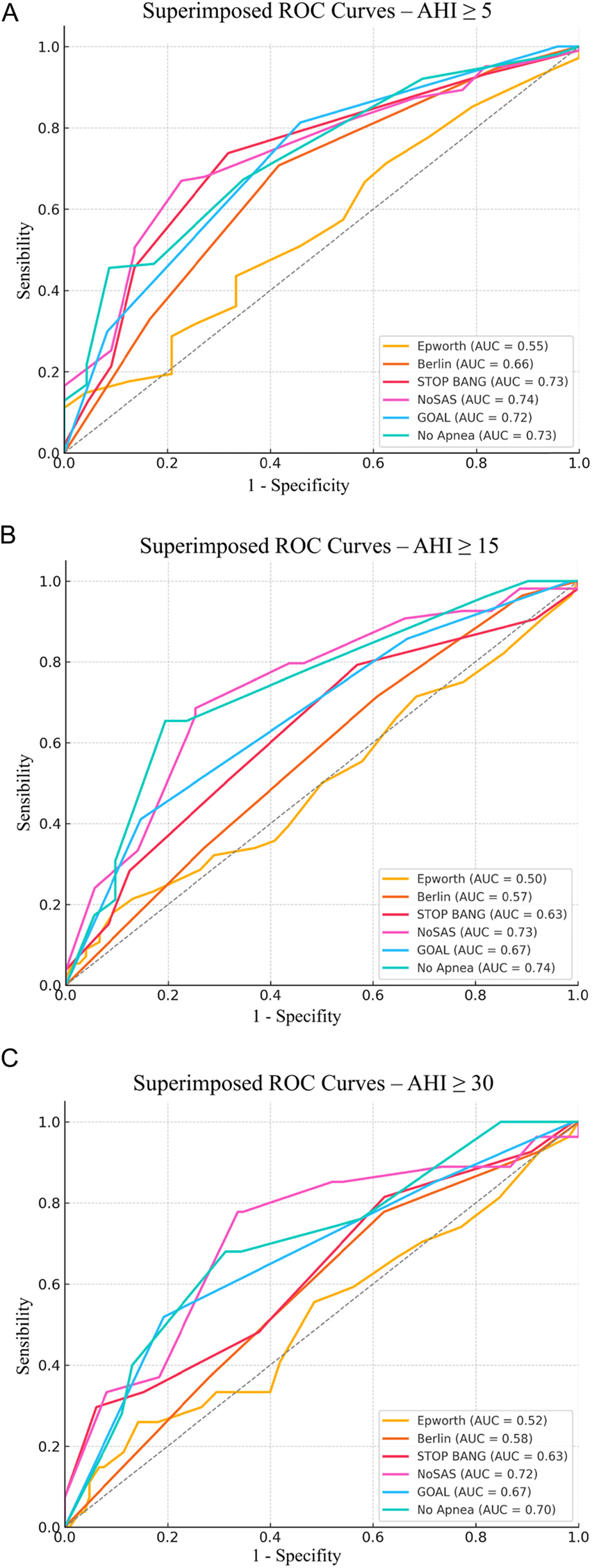
For diagnostic performance, we calculated sensitivity, specificity, and area under the curve (AUC) for each score, and assessed diagnostic concordance using observed agreement and Cohen’s kappa.
AUCs were tested with the Mann–Whitney U test and compared using the DeLong test.
For association analyses, univariate analyses included Student’s t-tests for normally distributed quantitative variables, Mann–Whitney U tests for non-normal quantitative variables, and odds ratios using Fisher’s exact test for binary variables. Multivariate analyses were performed for anthropometric variables and comorbidities.
Missing data were handled by complete-case analysis (listwise deletion). All variables were also evaluated with AUC to compare their discriminative performance.
Ethical considerations
The study was conducted in accordance with the World Medical Association Declaration of Helsinki and was approved by the Institutional Review Board of the Centre Hospitalier Universitaire de Martinique (approval number 2023/032).
In accordance with French regulations, all participants received written information and provided informed consent to participate.

Comments (0)