Study population
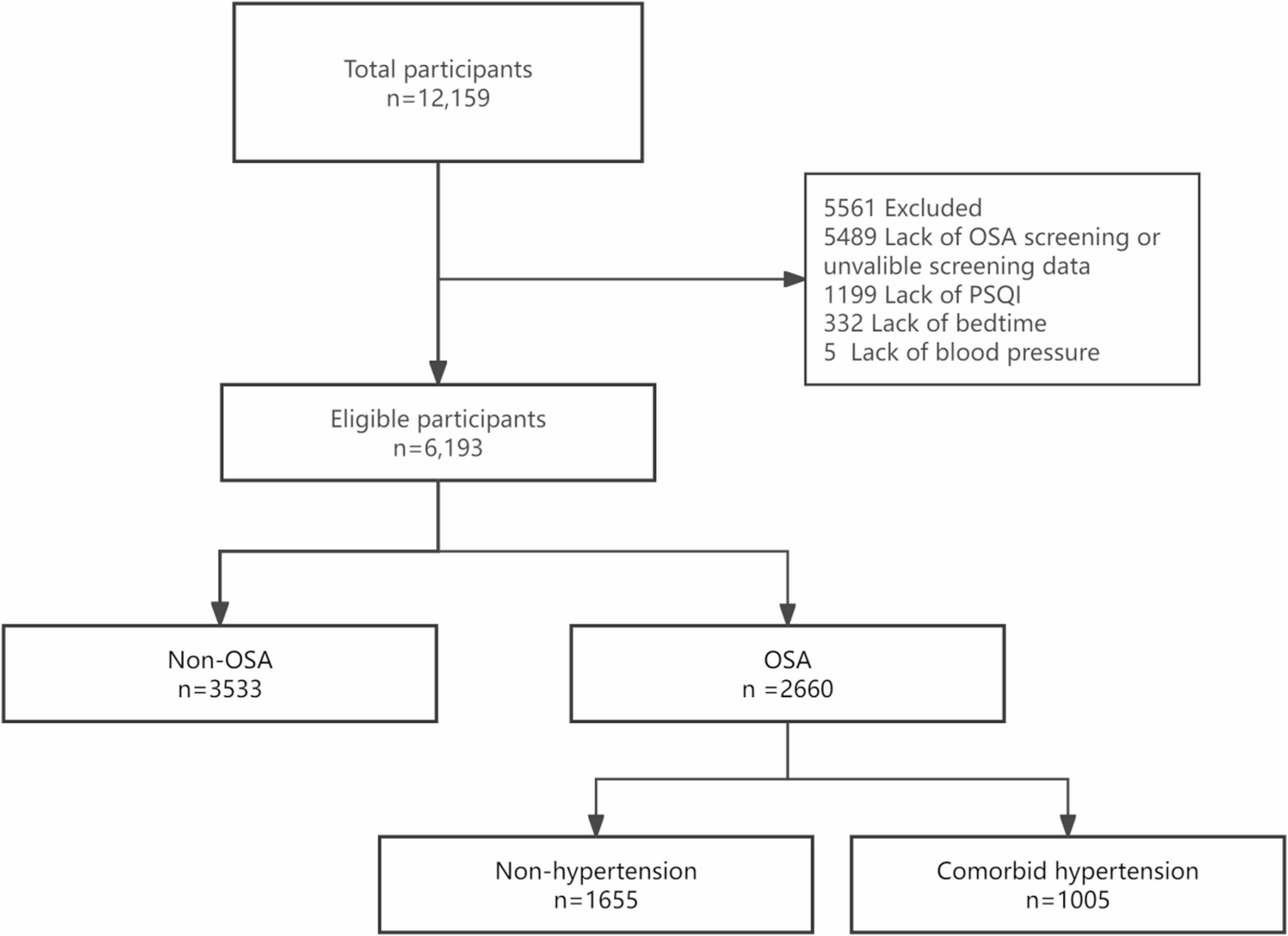
This cross-sectional study utilized baseline data from the Guangdong Sleep Health Study (GSHS) and the National Health Survey (CNHS) in Guangdong Province, China [12, 13].
The CNHS (2012–2017) was a nationwide, stratified multistage cluster survey of adults aged 20–80 years designed to establish reference intervals for physiological constants and determinants of noncommunicable diseases [12]. The GSHS is a community-based cohort in Guangdong Province that used multistage stratified cluster sampling to recruit permanent residents from selected districts in Shantou and Meizhou cities; the detailed protocol has been published elsewhere [13].
Participants were permanent residents aged ≥ 20 years at the time of the baseline survey. The study protocol was approved by the Ethics Committee of Guangdong Provincial People’s Hospital (Approval No. GDREC2020221H, KY-Z-2022-391-03), and all participants provided written informed consent.
Data collection
Data were collected through face-to-face questionnaires, physical examinations, and sleep monitoring. Trained staff administered questionnaires to capture demographic characteristics, socioeconomic status, medical history, and lifestyle factors (e.g., smoking, alcohol consumption, physical activity, dietary habits). Data quality was ensured through one-on-one interviews, reviewer verification, and double-entry data input. Physical measurements, including height and weight, were conducted in a fasting state.
Obstructive sleep apnea diagnosis
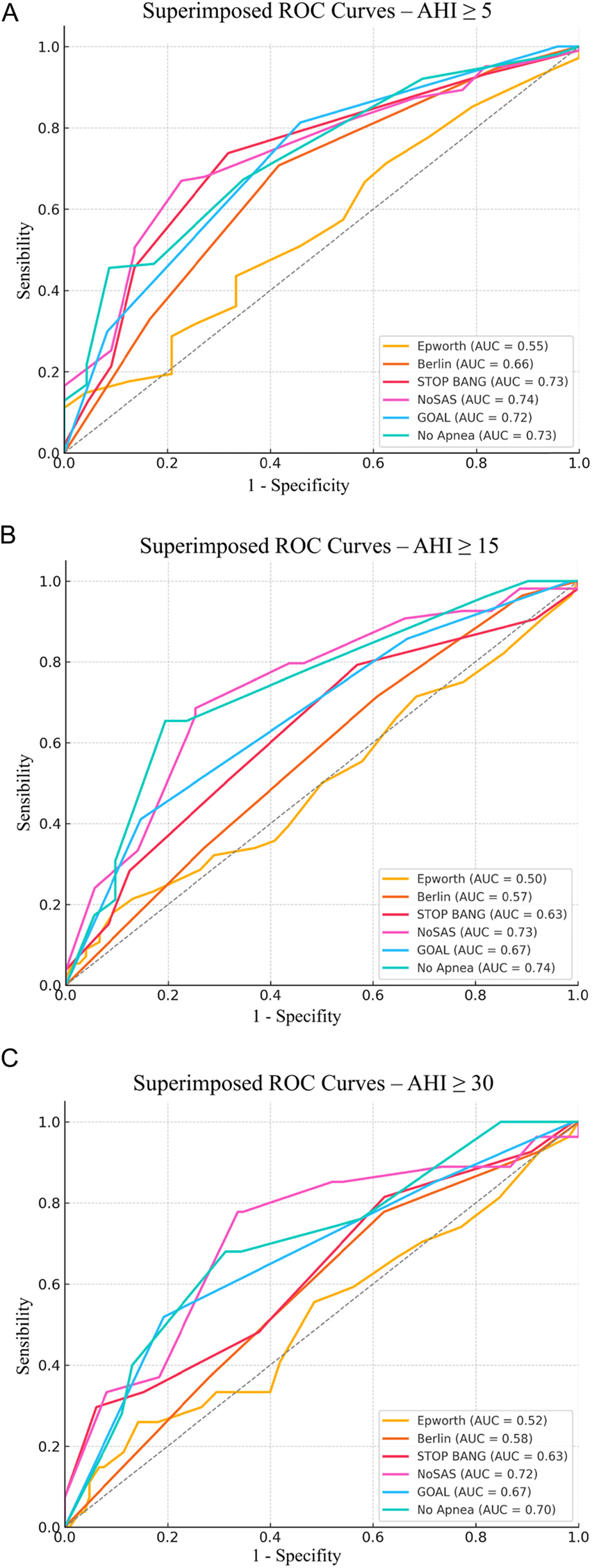
Obstructive sleep apnea (OSA) was diagnosed using a Type IV wearable intelligent sleep monitor (WISM; Chengdu Yunwei Kang Medical Technology Co., Ltd., Chengdu, China), which records oxygen saturation, pulse rate, and somatic movement signals overnight. This same device model was previously validated against simultaneous in-laboratory polysomnography by our group in 196 participants, demonstrating sensitivity/specificity of 93%/77% for AHI ≥ 5/h and 92%/89% for AHI ≥ 15/h [14]. OSA was defined as ≥ 5 oxygen desaturation events per hour [15].
Hypertension diagnosis
Blood pressure was measured using an electronic sphygmomanometer (Omron HEM-907, Omron, Japan) after participants rested for ≥ 5 min, following a period of fasting and the avoidance of medications that could affect blood pressure. Three consecutive measurements were averaged. Hypertension was defined as mean systolic blood pressure ≥ 140 mmHg, mean diastolic blood pressure ≥ 90 mmHg, current use of antihypertensive medication, or self-reported physician-diagnosed hypertension.
Assessment of sleep behavioral habits
Sleep behavioral habits were assessed via self-reported responses in a sleep questionnaire, using the Pittsburgh Sleep Quality Index (PSQI) and Insomnia Severity Index (ISI). The PSQI evaluated sleep quality over the past month, covering bedtime, sleep latency, duration, efficiency, disturbances, sleep medication use, and daytime dysfunction (score range: 0–21). The ISI assessed insomnia severity over the past week (score range: 0–28). Higher scores indicate poorer sleep quality. Bedtime was obtained directly from item 1 of the Pittsburgh Sleep Quality Index (PSQI), in which participants reported their usual bedtime over the past month (open-ended response in hours and minutes, e.g., “10:30 PM”). Responses were recorded in 24-hour format, standardized to Beijing time (UTC + 8) to account for any regional differences within the study area, and subsequently categorized into three groups for analysis: early (≤ 21:59), moderate (22:00–23:59), and late (≥ 00:00). Sleep duration was derived from PSQI responses, and sleep efficiency was calculated as (total sleep duration/total time in bed) × 100%. Participants were classified as using or not using sleep medications based on PSQI responses.
Data analysis
Data were analyzed using R software (version 4.3.2; R Foundation for Statistical Computing). Missing data were imputed using multiple imputation by the random forest method (mice package, version 3.16.0). Continuous variables were reported as means ± standard deviations, and categorical variables as counts (percentages). Multivariable logistic regression was used to examine the association between bedtime categories and hypertension, adjusting for potential confounders (e.g., age, sex, BMI, lifestyle factors). All tests were two-sided with a significance level of α = 0.05. Effect sizes were reported as odds ratios (ORs) with 95% confidence intervals (CIs). Pre-specified subgroup analyses were conducted stratified by age groups (20–44, 45–59, and ≥ 60 years) to explore potential heterogeneity.

Comments (0)