In the last two decades, ProACT device implantations have evolved as a surgical technique in treating PPI. It is widely established that surgical outcomes improve as a surgeon gains experience [26], a principle supported by earlier studies on surgical learning curves [27]. However, limited research has been done on the surgical learning curve of the ProACT implantation since Hübner et al. reported their findings in 2006 [16].
Learning curve analysis
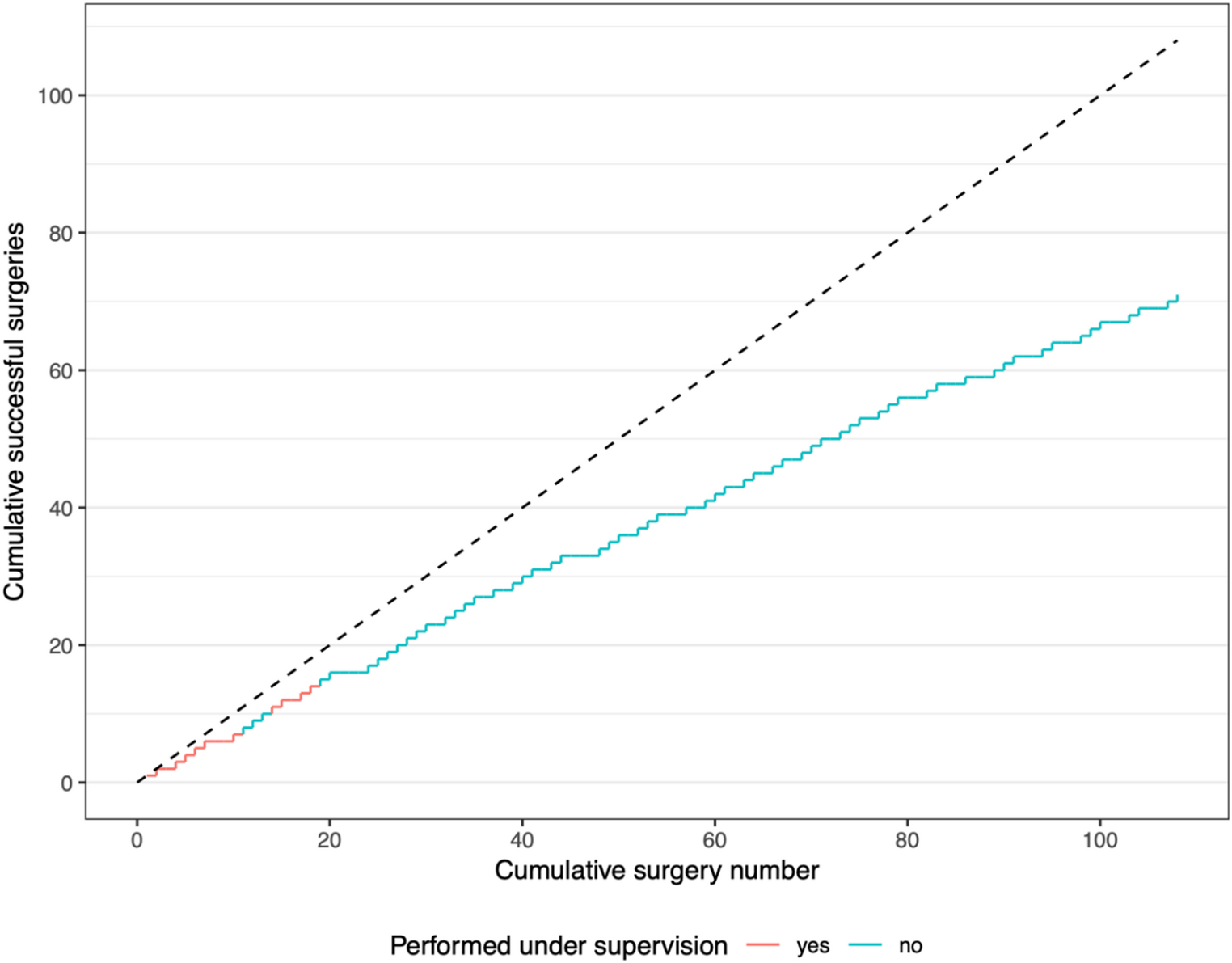
We found no statistically significant effect of surgical experience over a 5-year time period on surgical success rates, defined by postoperative continence. This suggests that for a consultant urologist, a supervised training period of approximately 15 surgeries is sufficient to achieve satisfactory operative results.
The observed absence of a learning curve differs from earlier results reported by Hübner et al. [16], who observed better results in their latter cohort.
One key difference may be that Hübner et al. conducted their research shortly after the introduction of ProACT, when surgical techniques and postoperative protocols were still evolving. During the current study, no such updates were made. Moreover, the surgeon in the current study was trained by a urologist highly proficient in ProACT implantation.
In some learning curve studies, operating time is used as an indicator of surgical proficiency. However, in ProACT implantations, the relatively short surgical time is influenced by factors beyond the surgeon’s skill, such as the experience of the surgical team and whether malfunctioning ProACT devices were simultaneously removed during surgery. While we observed a statistically significant difference in surgery times between the three outcome groups, we consider this difference clinically irrelevant. Notably, the ’dry’ group, with the shortest surgical time, also had less ProACT removals, which could explain this difference.
Efficacy and safety
Overall efficacy of ProACT in this study aligns with prior research, with 61% of patients achieving dryness and 81% achieving at least 50% improvement of continence. The most recent meta-analysis on this subject reported an overall dryness rate of 55%, with varying definitions of dryness across studies [11].
We only reported complications occurring in the first 6 months post-surgery, as this was the follow-up period available for all the patients included, resulting in a complication rate of 21%. In the literature, complication rates vary between 12% and 31% in meta-analyses [11, 14]. In our cohort, the intraoperative urethra/bladder perforation rate was 2.8%, lower than the meta-analyses estimate of 5.3% [15]. This supports the absence of a significant learning curve in this dataset, as it includes the first ProACT implantation surgeries performed by a surgeon and does not fall short of the outcomes reported in the literature.
Predictors of surgical success
Previous studies have shown that severe preoperative incontinence is a negative predictor for postoperative dryness [20, 21]. Our results confirm this, where a significant correlation between pre- and postoperative incontinence is noted. Our findings highlight the importance of patient selection and counseling. Instead of focusing on surgical experience, more attention should be given to identify preoperative predictors of success to optimize procedure outcomes.
However, ProACT can still be a viable option for patients with severe incontinence, since 47% of our patients with severe incontinence achieved dryness and a total of 78% experienced at least a 50% improvement in symptoms. In our study, only 14% of the patients who experienced a 50% reduction in incontinence (‘improved group’) had another treatment for their incontinence, opposed to 90% of patients who had no effect of the surgery. In this ’improved’ group, we observe a median subjective improvement of 80%. This indicates that, while this group does not achieve ’dryness’, they still have a clinically relevant effect of the ProACT implantation.
Reduced bladder compliance and detrusor overactivity are also highly correlated to PPI and most PPI patients do not have sheer stress incontinence, but also an urgency-incontinence component [28]. It has also been shown that successful ProACT treatment decreases bladder contractility parameters [20, 29]. In this study the UDS results showed reduced compliance in 26% of patients and detrusor overactivity in 59%. We recommend prospective research into preoperative predictors of success to optimize ProACT outcomes.
Study limitations
There are some limitations to this study. First, there was a limited duration of follow-up since our most recent patients were treated in 2024. Because of this, we were not able to report on long-term results of the ProACT device. A second limitation is that incontinence was primarily measured using patient-reported pad usage, as not all patients completed incontinence diaries. While pad usage is a widely accepted measure of continence [30], it is not standardized. Studies on the correlation between pad usage and actual urine loss in grams have yielded mixed results, with some showing strong correlation [31] and others recommending against its use for objective measurement [32]. At last, the analyzed learning curve only included one surgeon. It is plausible that interpersonal variation plays a role in learning curves. However, given that no clear trend is observed in the current data and the observed efficacy is comparable to results in previous literature, it seems unlikely that such variation would manifest in a significant learning curve in a larger group of surgeons. This is particularly true since the ProACT procedure is often performed by experienced urologists who are incorporating this specific intervention into their existing practice.

Comments (0)