This systematic review synthesizes the contemporary evidence on EP-HoLEP and demonstrates that selective anatomical preservation during enucleation can meaningfully improve rates of antegrade ejaculation compared with conventional HoLEP, while maintaining clinically relevant relief of lower urinary tract symptoms. Importantly, the reviewed literature indicates that ejaculatory preservation is not a binary outcome but is closely related to the extent and location of tissue spared during enucleation, reinforcing the importance of peri-ejaculatory anatomy in surgical planning. Preservation of sexual function, including ejaculation, is increasingly recognized as a relevant outcome in contemporary BPH management [1].
Traditionally, loss of AE after TURP has been attributed to impaired bladder neck closure. However, accumulating anatomical, histomorphological, and imaging data indicate that ejaculation depends on the coordinated function of peri-verumontanum, intraprostatic urethral, and sphincteric structures rather than bladder neck competence alone [6,7,8, 26]. This evolving understanding provides the conceptual foundation for contemporary EP-HoLEP strategies that seek to preserve key peri-ejaculatory anatomy during enucleation. These evolving physiological concepts are consistent with recent analyses emphasizing the functional importance of the ejaculatory hood, peri-verumontanal musculature, and sub-sphincteric emission mechanisms in contemporary BPH surgery [27].
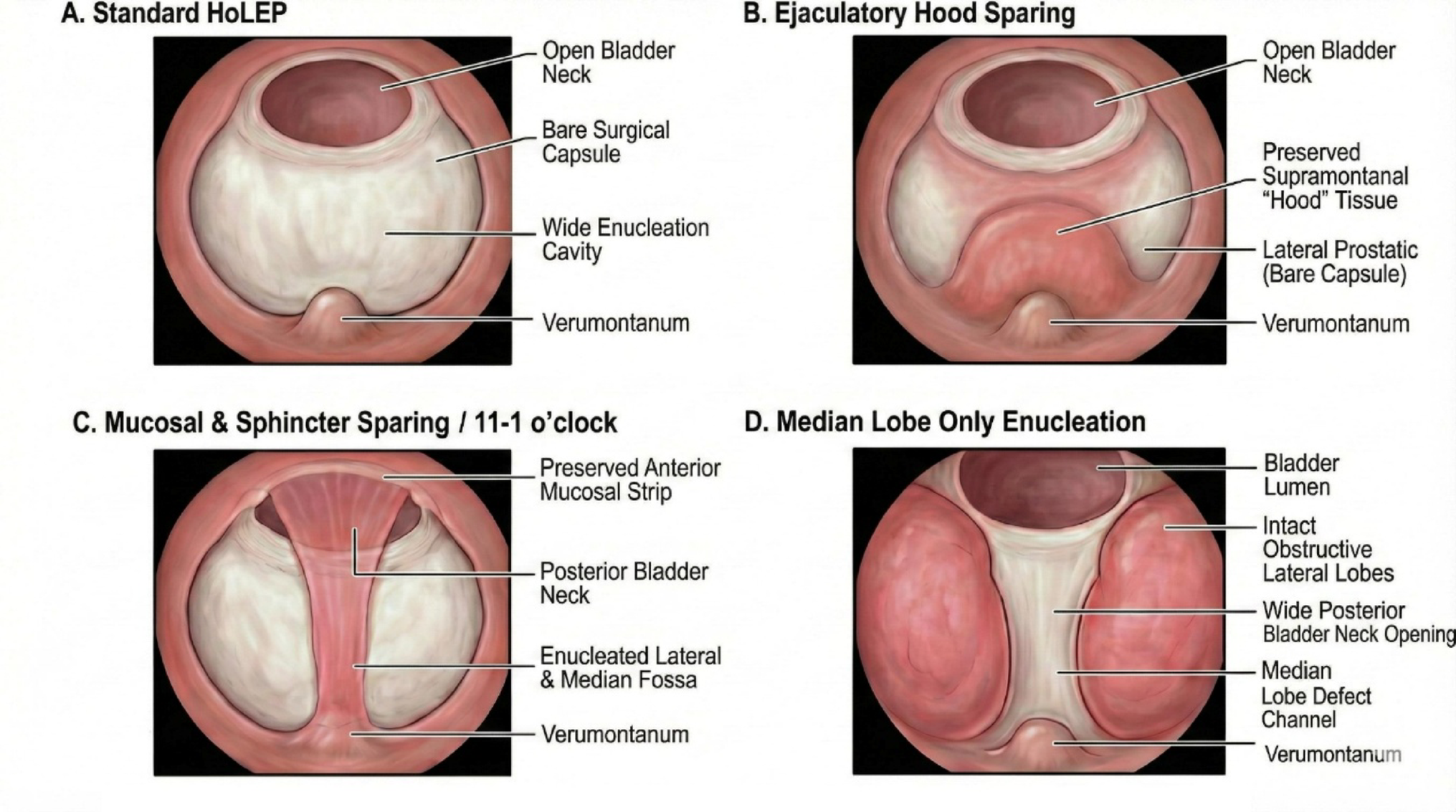
The heterogeneity of EP-HoLEP techniques identified in this review reflects differing surgical interpretations of which anatomical elements are most critical for ejaculation, rather than inconsistency in the underlying physiological concept. Early attempts at EP-HoLEP, particularly those limited to superficial ejaculatory hood or paracollicular mucosal sparing, yielded inconsistent results, likely because they preserved visible landmarks without adequately respecting the deeper muscular structures involved in emission and expulsion [16]. These early experiences highlight that preservation confined to the mucosal hood alone is insufficient and that effective ejaculation preservation requires a more anatomically informed modification of the enucleation plane.
More contemporary EP-HoLEP approaches—including modified two-lobe enucleation, urethral mucosa-sparing techniques, targeted bladder-neck preservation, and selective median-lobe enucleation—share a common principle of deliberate avoidance of dissection in regions closely associated with peri-verumontanum and proximal urethral sphincteric anatomy [17, 18, 22]. Rather than abandoning the enucleation concept, these techniques attempt to redefine the safe dissection boundaries within the prostatic urethra. Selective median-lobe HoLEP represents a distinct conceptual strategy, emphasizing anatomical patient selection rather than global modification of the enucleation technique, and illustrates that ejaculation preservation may be achievable by limiting surgical intervention in anatomically favourable prostates [20, 21]. However, such approaches may not be applicable across the full spectrum of prostate morphologies and instead underscore the importance of a patient-based approach that integrates individual anatomical configuration, prostate morphology, and patient priorities when selecting an ejaculation-preserving strategy.
An additional and clinically relevant contributor to this heterogeneity is prostate volume. When prostate volume distributions across the included studies are examined, the available evidence predominantly reflects outcomes in patients with moderate-sized glands, particularly in the 40–80 g range. Notably, only one randomized study explicitly defined a prostate volume inclusion criterion, while most others either did not report volume-based selection or included heterogeneous gland sizes without stratified analysis. This lack of standardized reporting likely contributes to the heterogeneity observed in ejaculatory and functional outcomes across studies and limits the generalizability of ejaculation-preserving HoLEP techniques, particularly to patients with large-volume prostates. In such cases, technical factors—including the feasibility of bladder neck preservation, the extent of tissue sparing, and maintenance of adequate enucleation planes—may differ substantially and influence both ejaculatory and urinary outcomes. Accordingly, prostate volume should be explicitly considered during patient selection and surgical planning, and future studies should incorporate volume-stratified analyses to better define the anatomical boundaries within which ejaculation-preserving HoLEP can be reliably applied.
A patient-based approach is therefore important when considering ejaculation-preserving HoLEP. Suitability for EP strategies depends on individual anatomy, prostate morphology, and patient priorities rather than a uniform set of criteria. From an anatomical standpoint, EP-HoLEP may be most feasible in men with relatively preserved peri-verumontanum and apical anatomy, a clearly identifiable surgical capsule, and prostate configurations that allow controlled dissection without extensive disruption of paracollicular structures. Patients with a dominant intravesical median lobe and limited lateral lobe obstruction may be particularly suitable for selective median-lobe approaches, whereas those with bulky circumferential adenomas or marked apical distortion may be less amenable to highly tissue-sparing techniques. Prostate size may also influence strategy selection; in moderate-sized glands, mucosal- and paracollicular-sparing techniques are often technically more manageable, whereas in very large prostates (e.g., > 100 g) extensive sparing can be challenging and may increase operative complexity. Beyond short-term functional outcomes, the durability of ejaculation-preserving approaches warrants careful consideration. Although these modifications can effectively maintain antegrade ejaculation in selected patients, they may involve important trade-offs that should be addressed during preoperative counseling, particularly the need to balance short-term sexual benefit against potential long-term functional outcomes.
In anatomically favorable prostates—especially those with a dominant intravesical median lobe—selective median-lobe enucleation can provide excellent early preservation of ejaculation and meaningful symptom relief; however, by intentionally narrowing the enucleation field, this approach may leave residual adenomatous tissue and has been associated in some series with higher rates of persistent LUTS and subsequent reintervention (up to 14.5%). Thus, the short-term advantage in ejaculatory preservation may, for a subset of patients, come at the cost of reduced durability of symptom relief.
In prostates without a dominant median lobe, a purely selective approach is generally less appropriate; in these cases, mucosal- and paracollicular-sparing strategies that preserve the peri-verumontanal region while allowing more complete lateral lobe enucleation may offer a more balanced compromise between ejaculation preservation and durable obstruction relief.
A similar balance applies to more complex mucosal- and paracollicular-sparing strategies (e.g., Double-n techniques). These approaches consistently improve ejaculatory outcomes compared with standard HoLEP, yet they are often associated with longer operative times and greater technical demands, which may limit broader applicability and could influence outcomes outside high-volume centers.
While ejaculation preservation has become an increasingly important patient-reported outcome, it must be balanced against operative efficiency, completeness of adenoma removal, and long-term durability. Several studies included in this review suggest potential trade-offs associated with EP-HoLEP, including longer operative times, reduced enucleated tissue weight, or higher retreatment rates in selected cohorts [18, 21, 22]. These findings indicate that ejaculation preservation may, in some cases, necessitate a narrower enucleation margin, reinforcing the need for careful patient selection and preoperative counselling.
Importantly, despite these trade-offs, most studies reported comparable short-term improvements in urinary symptom scores, maximum urinary flow rate, and continence outcomes between EP-HoLEP and standard HoLEP, consistent with broader HoLEP literature demonstrating the robustness of enucleation-based relief of obstruction [29, 30, 2]. In addition, refinements in HoLEP technique have been associated with improved perioperative recovery profiles—such as earlier catheter removal—supporting the broader feasibility of anatomically mindful modifications [28]. Ultimately, the choice of EP-HoLEP should be individualized through shared decision-making that explicitly balances anatomical feasibility, expected urinary benefit, durability of symptom relief, and the patient’s valuation of ejaculatory preservation. In addition, wider dissemination of HoLEP in general—and EP-HoLEP in particular—may be constrained in some settings by the need for specialized laser equipment, morcellation systems, and associated costs.
The overall quality of evidence is moderate but evolving. Although randomized and prospective comparative studies suggest a consistent signal favouring EP-HoLEP for preservation of AE, much of the available literature consists of single-centre studies with heterogeneous technique definitions, variable follow-up, and inconsistent assessment of sexual outcomes. Risk-of-bias assessment identified frequent concerns related to patient selection, deviations from intended interventions, and outcome measurement, particularly in retrospective cohorts. These limitations preclude definitive conclusions regarding the superiority of any single EP-HoLEP technique and highlight the need for standardized reporting. Taken together, these findings align with contemporary guideline emphasis on functional outcomes and patient-centred decision-making in BPH surgery.
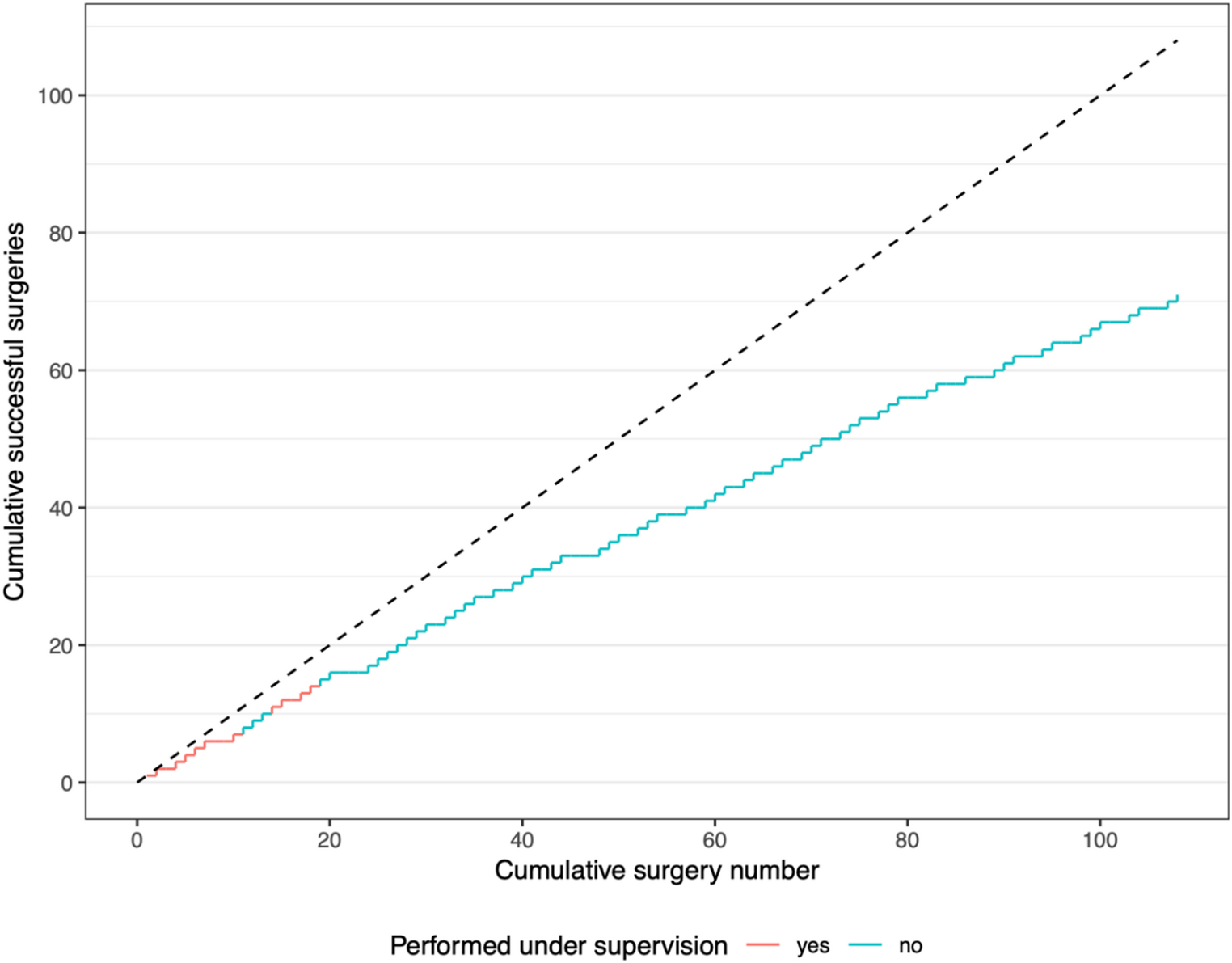
Several limitations of this systematic review should be acknowledged. First, substantial heterogeneity in study design, surgical technique, and outcome definitions — particularly regarding ejaculatory outcomes — precluded quantitative meta-analysis. Second, definitions of ejaculation preservation varied across studies, and validated sexual function questionnaires were not uniformly employed. Many reports relied on subjective or non-standardized categorizations of ejaculation (e.g., ‘preserved,’ ‘reduced,’ or ‘absent’) rather than validated instruments such as the MSHQ-EjD-SF or structured semen analyses. This methodological variability likely introduces reporting bias and limits the reliability and comparability of ejaculatory outcomes across studies. Third, follow-up duration was limited in many reports, restricting assessment of long-term durability and retreatment risk. This review was intentionally limited to ejaculation-preserving modifications of HoLEP; therefore, other contemporary surgical techniques such as Aquablation or ThuLEP were not systematically evaluated. Although emerging data suggest favorable ejaculatory outcomes with various techniques in selected patients, direct comparisons with HoLEP remain limited and heterogeneous. Finally, most included studies originated from high-volume centres with significant HoLEP experience, which may limit generalizability to broader practice settings. These technically demanding modifications are also likely subject to a steeper learning curve, which may partly explain why most published series originate from high-volume centers.
In summary, the available evidence supports the anatomical plausibility and surgical feasibility of ejaculation preservation during HoLEP in selected patients. Rather than representing a single standardized procedure, EP-HoLEP encompasses a spectrum of anatomically informed adaptations aimed at minimizing disruption of peri-ejaculatory structures while retaining the benefits of enucleation. Future studies with standardized technique definitions, validated outcome measures, and longer follow-up are required to define the optimal balance between ejaculation preservation, functional efficacy, and long-term durability.

Comments (0)