Pediatric urolithiasis, despite being thought of as an uncommon condition, is becoming increasingly common and significant. According to many recent studies, urolithiasis is becoming more prevalent, especially over the last 25 years [20]. Importantly, almost 50% of pediatric urolithiasis patients recur within 3 years of their first stone episode [21]. All pediatric stone formers are considered a high-risk group among urolithiasis patients due to their high recurrence rate. Following the first stone episode, all children should have a thorough metabolic evaluation performed, according to the most recent American and European guidelines [7, 9].
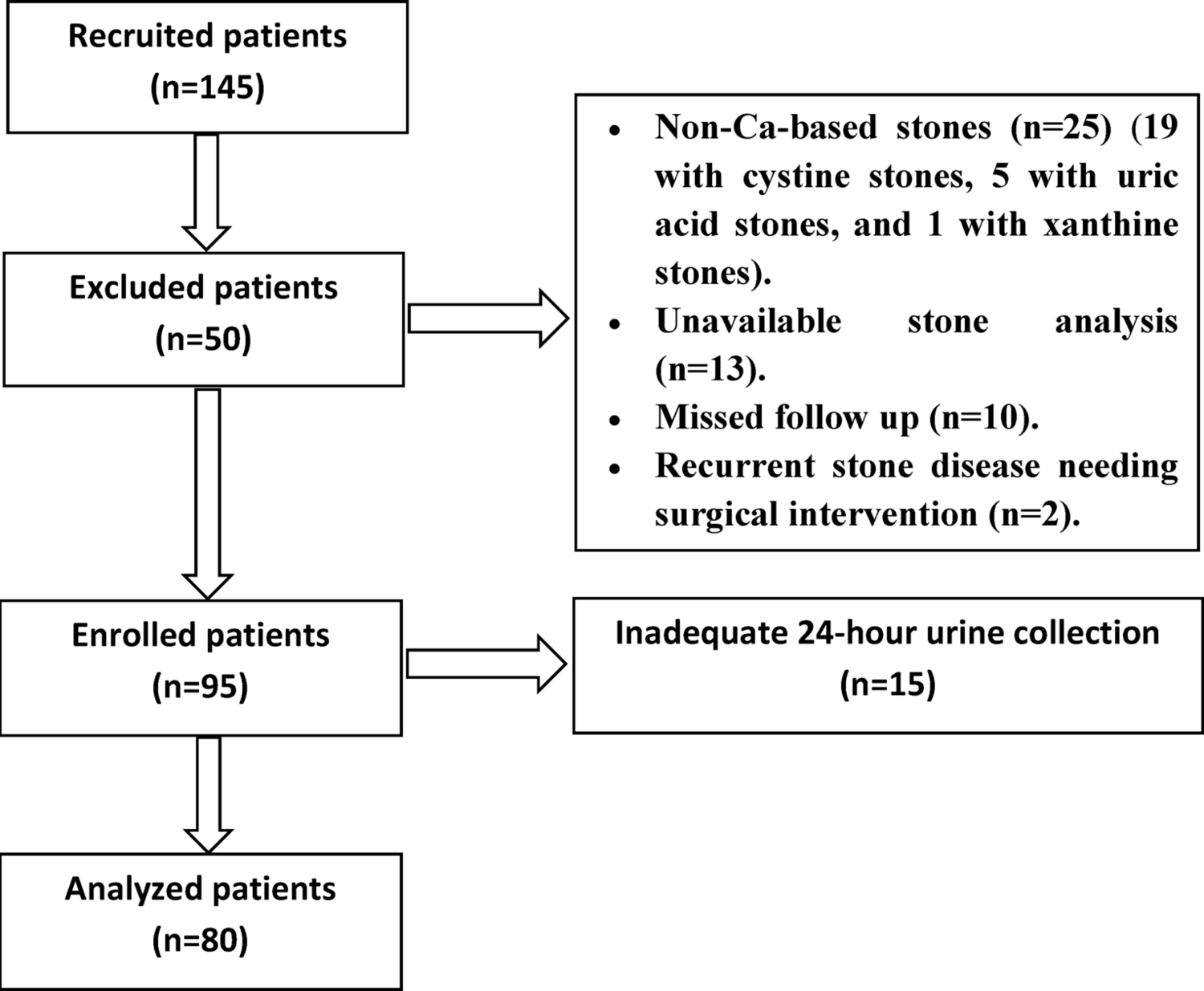
In this study, we hypothesized that not all children are at high-risk for stone disease recurrence, and routine metabolic evaluation could be refined to include only a high-risk subgroup of pediatric population based on certain patient and stone characteristics. Therefore, we recruited children with history of intervention for calcium-based stone disease. Full metabolic evaluation, including serum and 24-hour urine studies, was performed for included patients.
Regarding the usefulness of serum metabolic assessment in the context of urolithiasis and its relationship to recurrence risk, no consensus has been reached. Serum tests are usually obtained to assess renal function and calcium metabolism. The clinical utility of these tests has been questioned, though, because children with nephrolithiasis rarely have abnormal serum studies [22]. Albeit, serum chemistries that may indicate underlying medical disorders associated with stone disease include creatinine, electrolytes, calcium and uric acid [9].
In a study conducted by Bevill et al. to evaluate metabolic abnormalities in a pediatric population after their first stone episode, a retrospective review of 113 children was performed. Their demographic data, serum and 24-hour urine chemistry results and treatments were compared. When serum chemistry results were evaluated, the likelihood of having serum metabolic abnormalities was very low; and none of the detected abnormalities needed further evaluation or treatment. Hypo- and hypercalcemia were present in 4% and 6% of patients, respectively. Hypo- and hyperphosphatemia were present in 1% and 12%, respectively. Hyperuricemia was present in 4% [22].
In other studies that assessed serum metabolic abnormalities, most patients also had serum chemistry results within normal range. Hypercalcemia, hyperuricemia, and hyperphosphatemia were noted in 2–14%, 3–9% and 2–4%, respectively [23, 24]. To date, no studies have investigated the association between metabolic acidosis and kidney stone formation [25].
In our study, abnormal serum chemistry was present in 25 patients (31.25%). The frequency of relevant metabolic abnormalities was as follows: high serum creatinine (3.75%), hypocalcemia (8.75%) (after correction of serum calcium for hypoalbuminemia), hypo- and hyperphosphatemia (3.75% and 5%, respectively), hyperuricemia (6.25%), metabolic acidosis (12.5%) and metabolic alkalosis (1.25%). These results cope with other studies apart from absence of hypercalcemia in our study population; mostly due to a common, yet non-indicated, practice of dietary calcium restriction.
Regarding 24-hour urinary metabolic abnormalities, hypercalciuria is found in 30–50% of calcium stone formers, making it the most common metabolic abnormality in stone disease patients. Hyperoxaluria is found in 5–30%, hyperuricosuria in 10–40%, and hypocitraturia in 10–50% of patients [26, 27]. Many studies have been conducted to limit the 24-hour urinary metabolic evaluation to assess the metabolites whose abnormalities are of the highest prevalence among stone formers. In the study conducted by Bevill et al., 24-hour urine chemistry results revealed that 99 patients (88%) had at least one abnormal metabolite. This study differs from previous literature findings by identifying a low rate of hypercalciuria and hyperoxaluria (11% and 15%, respectively) and a high rate of low urine volume and hypocitraturia (89% and 68%, respectively), suggesting a change in metabolic abnormalities associated with modern pediatric stone disease [22].
Chan et al. proposed a simplified approach to metabolic evaluation in first-time stone formers with a stone analysis available. A limited urinary metabolic evaluation consisting of four parameters (24-h calcium, citrate, and oxalate and low urinary volume) was compared to a complete urinary metabolic evaluation. These four parameters were selected being the most prevalent metabolic abnormalities reported by previous studies. The number and type of metabolic abnormalities that would have been missed with this limited evaluation were determined. The most common abnormalities were hypocitraturia (69.6%), low urine volume (52.5%), and hypercalciuria (22.5%). Hyperoxaluria and hyperuricosuria were present in 15% and 2.5%, respectively. High pH was present in 33.8% and low pH was present in 15%. A limited urinary metabolic evaluation was then able to detect the most significant metabolic abnormalities. Using this approach, metabolic evaluation can be simplified, and health care costs can be reduced [28].
In a study conducted on an Egyptian population, evaluation of metabolic abnormalities in 24-hour urine revealed metabolic abnormalities in 34 children (23%); with hypercalciuria and hyperoxaluria being the most common (41% and 32%, respectively). Hyperuricosuria and hypocitraturia were present in 21% and 6%, respectively [29].
In our study, abnormal 24-hour urine chemistry was present in 59 patients (73.75%). The frequency of these metabolic abnormalities among our study population was as follows: hypercalciuria (35%), hyperoxaluria (33.75%), low urine pH (31.75%), hyperuricosuria (12.5%), hypocitraturia (7.5%), and low urine volume (3.75%). The main difference from literature was in the prevalence of low urine volume and hypocitraturia; being less in our study population. This difference may be explained by ethnic, dietary, and therapeutic factors.
All the previous trials were on the side of 24-hour urinary metabolic evaluation aiming at finding a simplified or modified approach to overcome its drawbacks. However, another way to get over these drawbacks, we can still utilize 24-hour metabolic evaluation but limit it to a specified group among pediatric stones formers. This group should hence be discriminated from the whole pediatric urolithiasis population by certain risk factors. So, in this study, the results of serum and 24-hour urinary metabolic evaluation were tested for association with relevant patient and stone characteristics and were analyzed in relation to them. This approach aiming at modifying metabolic evaluation for pediatric urolithiasis wasn’t utilized in any previous studies. Unfortunately, the results of our analysis failed to identify such a high-risk group. None of the assessed patient and stone characteristics revealed a significant association with abnormal groups of serum, 24-hour urine or combined serum and 24-hour urine metabolic evaluation.
We also assessed recurrence risk for possible association with patient and stone characteristics, and with serum and urinary metabolic abnormalities. To date, most studies describe factors contributing to de novo urolithiasis; however, factors related to recurrence risk were also assessed in a few publications. In a retrospective study by De Ruysscher et al. to identify risk factors associated with recurrent nephrolithiasis in pediatric population, patient characteristics, presenting symptoms, medical history, laboratory results and management strategy (conservative vs. surgical) were analyzed. Only immobilization and need for surgical intervention were associated with a higher risk of stone recurrence in univariate, but not in multivariate analysis [30].
In another study by DeFoor et al., there was a significant difference in urinary calcium and citrate levels between children with de novo and recurrent calcium-based stone disease [31]. However, in a multi-center, multi-model, externally validated machine-learning study, routine urinary metabolic evaluation didn’t accurately predict stone type nor recurrence in nephrolithiasis patients [32].
Our results cope with those of De Ruysscher et al. and machine-learning study regarding the association between metabolic abnormalities and recurrence risk. However, immobilization, as a risk factor, was not assessed in our study. Management strategy (conservative vs. surgical) also couldn’t be assessed as our study included only patients who had surgical intervention. Stone characteristics were not previously explored as a risk factor for stone disease recurrence, to our knowledge. In our study, some stone characteristics (including stone volume, number, location, and laterality) had a significant association with the risk of recurrence in univariate analysis. However, in multivariate analysis, only stone laterality revealed such a significant association. Identifying a subgroup with high recurrence risk will help to provide them with more intense follow-up after the first stone episode.
After all, our findings were based on a small study population with a non-prospective, non-controlled design. Also, repeating 24-hour urine collection is recommended by guidelines to reflect metabolic variability and overcome dietary effects; however, in view of poor patient recruitment and compliance, and due to limited resources, 24-hour urinary metabolic evaluation was performed only once. So, we recommend that relevant patient and stone characteristics could be further assessed at a larger scale, prospective, controlled trials hoping to find a significant association between any of them and serum and urinary metabolic abnormalities. Furthermore, regarding recurrence risk, the follow-up period for some children might not have been long enough to observe all possible recurrences.

Comments (0)