This study found that among patients with obesity who underwent laparoscopic sleeve gastrectomy, those with a BMI ≥ 40 kg/m2 had a higher pain tolerance threshold than those with a BMI of 30 kg/m2 ≤ BMI < 40 kg/m2. After adjusting for confounding factors including sex, hypertension, and OSA, BMI still had a significant impact on the pain tolerance threshold. Although there were no statistically significant differences in BPI or NRS scores between the two groups after surgery, despite similar pain scores, the severe obesity group required less analgesia, with fewer presses of the PCA pump and less cumulative consumption of analgesic drugs postoperatively than the O group.
With the global rise in obesity, an increasing number of patients with obesity are undergoing surgery, presenting unique challenges in perioperative pain management due to their physiological traits. Particularly, patients with severe obesity often have OSA, with a prevalence of 60–70% that increases with BMI [21]. These patients are sensitive to sedatives and at higher risk for opioid-induced respiratory depression [22]. Effective pain management must balance analgesia with the risk of ventilatory issues. Understanding obesity's impact on pain can enhance postoperative treatment, improving safety and reducing perioperative complications.
Obesity is recognized as a low-grade inflammatory condition linked to the function of white adipose tissue [23]. As an endocrine and immune-active organ, fat tissue consistently emits pro-inflammatory cytokines throughout the body [24]. Compared to individuals with normal weight, those with obesity exhibit elevated levels of neutrophils and inflammatory cytokines (such as TNF-α, IL-1β, IL-6, IL-8) [25], which influence both the peripheral and central nervous systems, contributing to both acute and chronic pain [26, 27]. There is substantial evidence indicating that obesity is linked to various forms of chronic pain, including musculoskeletal pain, foot pain, osteoarthritis, low back pain, and systemic pain related to pain sensitization [28,29,30,31]. However, the relationship between obesity and postoperative acute pain is still debated. In gynecological surgery, women who were overweight or obese faced a notably higher risk of postoperative pain than those with a normal BMI [32]. Conversely, in inguinal hernia surgery, higher BMI was not associated with higher postoperative pain [11]. In joint replacement surgery, BMI was positively linked to IL-1β, IL-6, and TNF-α levels, but obesity did not correlate with increased pain or analgesic use within 24 h postoperatively [33].
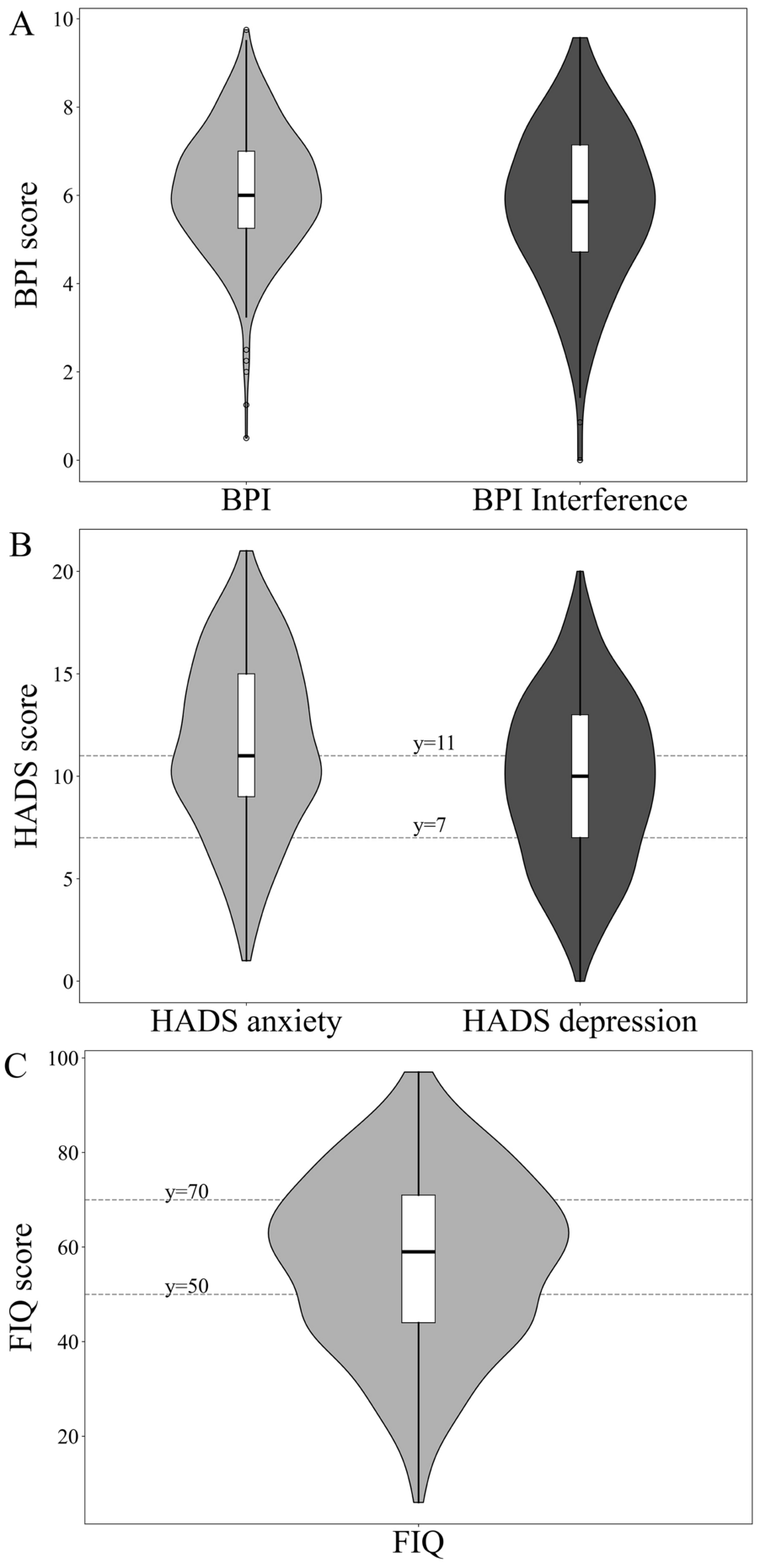
To enhance the accuracy of postoperative pain level assessment, this study employed both the single-dimensional NRS and the multidimensional BPI. The NRS, as a straightforward and rapid tool, facilitates the quick evaluation of pain intensity. However, its lack of comprehensiveness may result in issues such as inappropriate analgesic consumption [34, 35]. Recent research underscores the importance of function-based pain assessment in the postoperative context [36]. The BPI, in contrast to the NRS, offers a more comprehensive and standardized evaluation by incorporating multidimensional assessments, including pain severity and its impact on daily activities [20]. In this study, no statistically significant differences were observed in BPI and NRS scores between the O group and SO group. The absence of significant differences in preoperative baseline inflammatory cytokine levels between the two groups, coupled with the administration of a standardized multimodal analgesic regimen postoperatively to both, may collectively explain why no differences were observed in subjective pain scores (e.g., BPI, NRS). Both groups existed in a comparable baseline pro-inflammatory state and received analgesic interventions of comparable anti-inflammatory intensity, thereby achieving similar effects at the level of pain perception. Nevertheless, since all patients utilized postoperative PCA, they could alleviate pain by activating the analgesic pump when experiencing postoperative discomfort. By comparing the opioid and nonsteroidal anti-inflammatory drugs (NSAIDs) utilized in the postoperative analgesic pumps, it was observed that the frequency of PCA presses was significantly lower among the SO group than the O group, indicating that patients with severe obesity had a lower demand for analgesia. In summary, both groups achieved comparable pain relief (no difference in NRS/BPI scores) under our analgesic protocol, but patients with severe obesity did so with significantly less opioid/NSAID consumption, indicating a higher pain tolerance or lower analgesic requirement. Of course, the reduction in pain medication use in the SO group was based on clinical observations in the study. Due to significant baseline imbalances between the two groups, especially in the severe obesity cohort, a higher proportion of patients were male and had comorbidities such as OSA and hypertension, and sex and specific comorbidities are known to affect pain perception and analgesic medication need. They thus represent a potential confounder of the observed differences in opioid demand. Future prospective studies with larger sample sizes or balanced study groups, or specifically designed to adjust for these key demographic and clinical variables are needed to confirm and quantify the independent effect of BMI stratification on the need for postoperative analgesics.
Obesity is typically associated with heightened pain sensitivity and changes in pain threshold [37]. However, the association between pain sensitivity and BMI has yielded inconsistent and even contradictory results in both animal and human research. While some studies suggest that obesity may lead to hyperalgesia, others indicate reduced pain sensitivity or show no significant change [38]. This suggests that their relationship is likely not a simple linear one. In our study, the pain tolerance threshold of patients with severe obesity was higher than that of patients with obesity. These findings are consistent with Dodet et al. [39], who found higher pain thresholds in patients with higher BMI. In addition, a study by Blom-Høgestøl et al. [40] found that 2 years after bariatric surgery, the decrease in BMI, the improvement in physical health and activity ability, and the increase in social acceptance led to an increase in patient enjoyment, which resulted in decreased pain tolerance and increased pain sensitivity. This may explain the lower pain tolerance threshold in patients with obesity. With successful weight loss, anxiety is improved, psychological pleasure is increased, and patients' overall expectations of health and pain expectations are also increased [41], which may reduce the tolerance threshold for discomfort [42], rather than the physiological enhancement of pain perception itself. This highlights the critical moderating role of psychological and cognitive factors in pain experience and highlights the need for further research to elucidate the interplay between physiological and psychological mechanisms during weight change.
This study compared the levels of postoperative inflammatory cytokines in both groups of patients. Generally, the postoperative pain sensitivity of patients is significantly correlated with the levels of pro-inflammatory cytokines (such as TNF-α and IL-6, IL-1β) and anti-inflammatory cytokines (IL-10) in the serum [10, 43, 44]. However, the use of the NSAIDs (flurbiprofen axetil) after surgery in this study inhibited the expression of pro-inflammatory cytokines. In the O group, the cumulative consumption of flurbiprofen axetil was greater than that in the SO group. Therefore, the level of TNF-α was significantly lower in the O group. In addition, a decreasing trend in postoperative serum levels of TNF-α and IL-6 was observed. This pattern is likely attributable to the administration of NSAIDs via the PCA pump, which was routinely maintained for 48 h after surgery. As established cyclooxygenase inhibitors, NSAIDs possess anti-inflammatory properties that can suppress the production of pro-inflammatory cytokines such as TNF-α and IL-6 [45]. Consequently, cytokine levels decreased on postoperative day 1, whereas they showed a rebound after PCA discontinuation on postoperative day 3. Both groups of patients used multimodal analgesia including NSAIDs, nerve block analgesia, and PCA. The median NRS scores at each time point after surgery in both groups were < 4, and the QOR-15 scores at 24 h and 48 h after surgery showed no statistically significant differences.
This study has several limitations. First, a control group comprising patients with normal BMI was not established. Previous studies have compared the differences in postoperative pain between patients with obesity and patients without obesity. This study mainly focused on the comparison between patients with obesity and severe obesity. Second, the overall sample size was relatively small, and there were some confounding factors. These confounding factors were corrected through regression analysis, but there may be residual confounding from unmeasured variables. Third, the study observed multiple outcomes and lacked multiple adjustment. The findings should be considered preliminary and need to be confirmed in future studies. In addition, the pain tolerance threshold of patients may be related to psychological factors. We did not assess pain expectations of patients with different BMI and their preoperative anxiety states and pain catastrophizing. Future studies with large sample sizes are still needed to explore the correlation between psychological factors related to obesity and postoperative pain in patients with obesity. Fourth, this was a single-center study with primary outcomes focused on the short-term period (within 48 h postoperatively). This design limits the generalizability of our findings to other clinical settings and to longer-term recovery phases. Future multicenter studies with extended follow-up are warranted to validate our observations. Fifth, all patients in this study received a standardized, potent multimodal analgesic regimen, including bilateral paravertebral nerve blocks. While effective for pain control, this protocol itself may have attenuated potential intergroup differences. Consequently, the generalizability of our results to clinical contexts where regional blocks are not routinely employed may be limited. Finally, due to the nature of the grouping (based on BMI), blinding of patients and some research personnel was not feasible. Although this does not affect the primary objective measures (analgesic consumption, cytokine levels), the lack of blinding may have introduced measurement bias for some subjective pain assessments.
Based on the findings and limitations of this study, future work could explore the following aspects in greater depth: First, prospective studies should systematically incorporate assessments of psychological factors such as anxiety, pain expectation, and pain catastrophizing to clarify their mediating role in the differences in pain tolerance among patients with obesity. Second, considering the unique pharmacokinetic profile of patients with obesity, future research could explore individualized analgesic dosing models based on body weight or BMI to optimize efficacy and reduce adverse reactions. Ultimately, integrating patients' physiological indicators (inflammatory profile, genetic polymorphisms), psychological state, and social factors to construct a multimodal predictive model will be key to achieving truly precision and personalized postoperative pain management.

Comments (0)