
Remember me
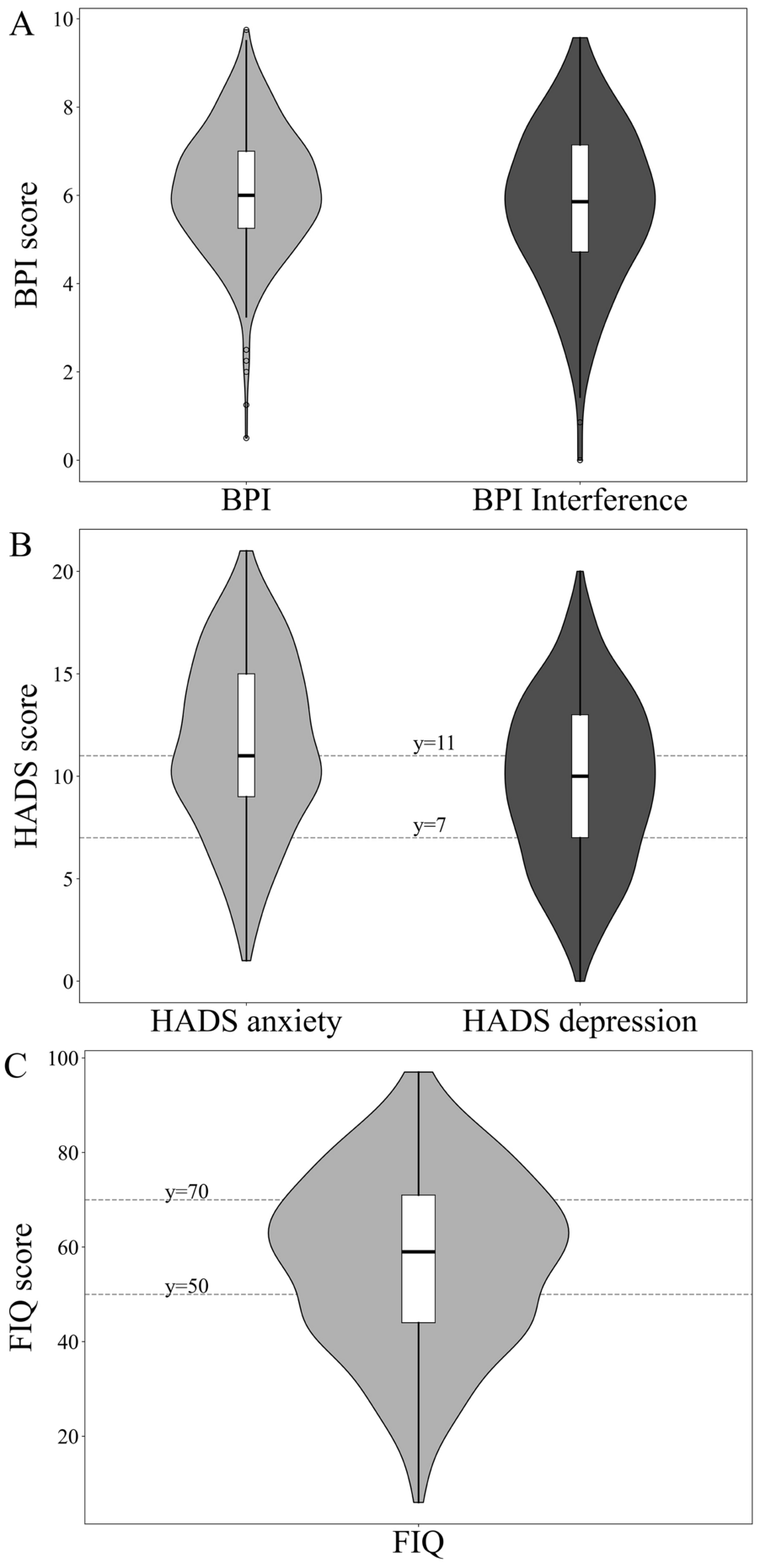
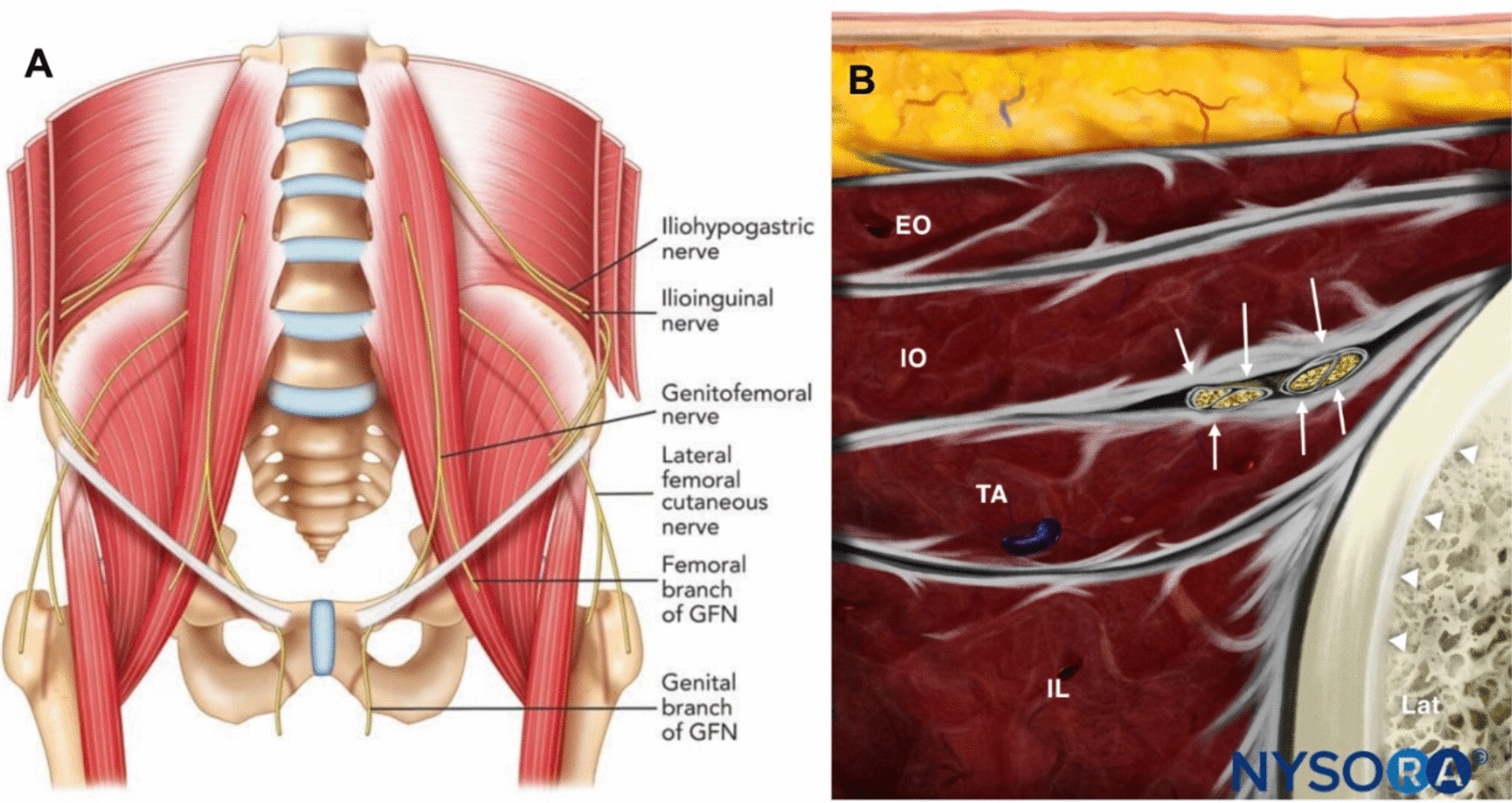
The IIN originates predominantly from the ventral ramus of the L1 spinal nerve, with occasional contributions from T12 [19, 20]. It arises at the lateral border of the psoas major, travels anteriorly across the quadratus lumborum, and pierces the transversus abdominis muscle near the iliac crest. The IIN then proceeds between the internal oblique and transversus abdominis muscles and closely accompanies the iliohypogastric nerve within the same fascial plane [20,21,22]. After passing between these muscles, it exits through the superficial inguinal ring, where it lies over the spermatic cord in male patients and the round ligament in female patients before giving off terminal branches to the mons pubis, labia majora or scrotum, and the upper medial thigh [19, 22] (Fig. 1).
Fig. 1 The alt text for this image may have been generated using AI.
The alt text for this image may have been generated using AI.(Source: NYSORA.com): Anatomy and ultrasound-guided localization of the ilioinguinal nerve (IIN) and iliohypogastric nerve. A Anterior view of the lumbar plexus branches in the lower abdomen and pelvis. The iliohypogastric and ilioinguinal nerves arise from the L1 nerve root, emerging from the lateral border of the psoas major muscle and coursing anterior to the quadratus lumborum between the layers of the abdominal wall (GFN indicates genitofemoral nerve). B Cross-sectional illustration demonstrating the typical location of the iliohypogastric nerve and the IIN (arrows) between the internal oblique (IO) and transversus abdominis (TA) muscles. (EO indicates external oblique; IO indicates internal oblique; TA indicates transversus abdominis; IL indicates iliacus; Lat indicates lateral direction) [32]. Reproduced from NYSORA (NYSORA—World Leader in Anesthesiology Education) under their educational image use policy
Cadaveric studies have demonstrated substantial anatomical variation in the IIN, mainly due to its origin, branching pattern, and anatomical relationship to the ASIS [20, 23]. The nerve originates from L1 in about 65–100% of cases, but it may also share a common trunk with the iliohypogastric nerve before diverging near the iliac crest [20]. In most people, the nerve enters the abdominal wall above or below the iliac crest and travels within 2 cm of the ASIS, depending on anatomical variation [23, 24]. In approximately one-third of cadaveric anatomical specimens, the IIN perforates the external oblique aponeurosis before entering the superficial inguinal ring, which is a variation that is associated with increased risk during surgical procedures [20, 25].
Histological studies show that the IIN is composed predominantly of small myelinated and unmyelinated fibers, which is consistent with its sensory and mixed motor–sensory roles [26]. The nerve provides motor branches to the internal oblique and transversus abdominis, which aid in facilitating lower abdominal wall stability, and provides sensory branches to the skin of the groin, pubic region, and medial thigh [19, 25]. However, minor contributions to the rectus abdominis have been observed in a few cases, which indicates functional crossover with the iliohypogastric and genitofemoral nerves [24, 27].
Because the IIN runs superficially and extends across the lower abdomen, it is vulnerable to entrapment or injury during procedures such as inguinal hernia repair, appendectomy, cesarean delivery, and other abdominal surgeries [1, 19]. Entrapment of the nerve most commonly occurs 1–2 cm medial and inferior to the ASIS, specifically at a point where the nerve transitions from the muscular layers into the subcutaneous tissue; this change increases its susceptibility to compression or tethering [1, 28]. The resulting ilioinguinal neuralgia often produces a radiating neuropathic pain involving the groin, genital region, and proximal thigh [1, 29].
Ultrasound imaging and magnetic resonance (MR) neurography provide valuable tools for identifying the fascial plane of the IIN and adjacent structures. On ultrasound, the nerve appears as a hypoechoic oval fascicle between the internal oblique and transversus abdominis, near the deep circumflex iliac artery [21, 22, 30]. Color Doppler improves vessel distinction, and the ASIS serves as a consistent sonographic reference point [21, 22]. MR neurography provides detailed imaging of the IIN from its origin near the psoas to its terminal branches; this can aid in diagnosing and guiding interventions for chronic groin pain syndromes [31].
Anatomical variations, such as duplication, absence of a distinct trunk, or a shared origin with the iliohypogastric nerve, are observed in 25–35% of cadaveric specimens. These variations underscore the importance of precise localization before performing nerve-targeted interventions [20, 26, 32]. Hence, a clear understanding of these variations is essential to minimize procedural complications and optimize outcomes during ultrasound-guided RFA.
Ethical ApprovalThis technical report describes a procedural technique and summarizes previously published evidence without involving human participants or patient data. All information presented is derived from publicly available scientific literature. Therefore, ethical approval and informed consent were not required for this manuscript.
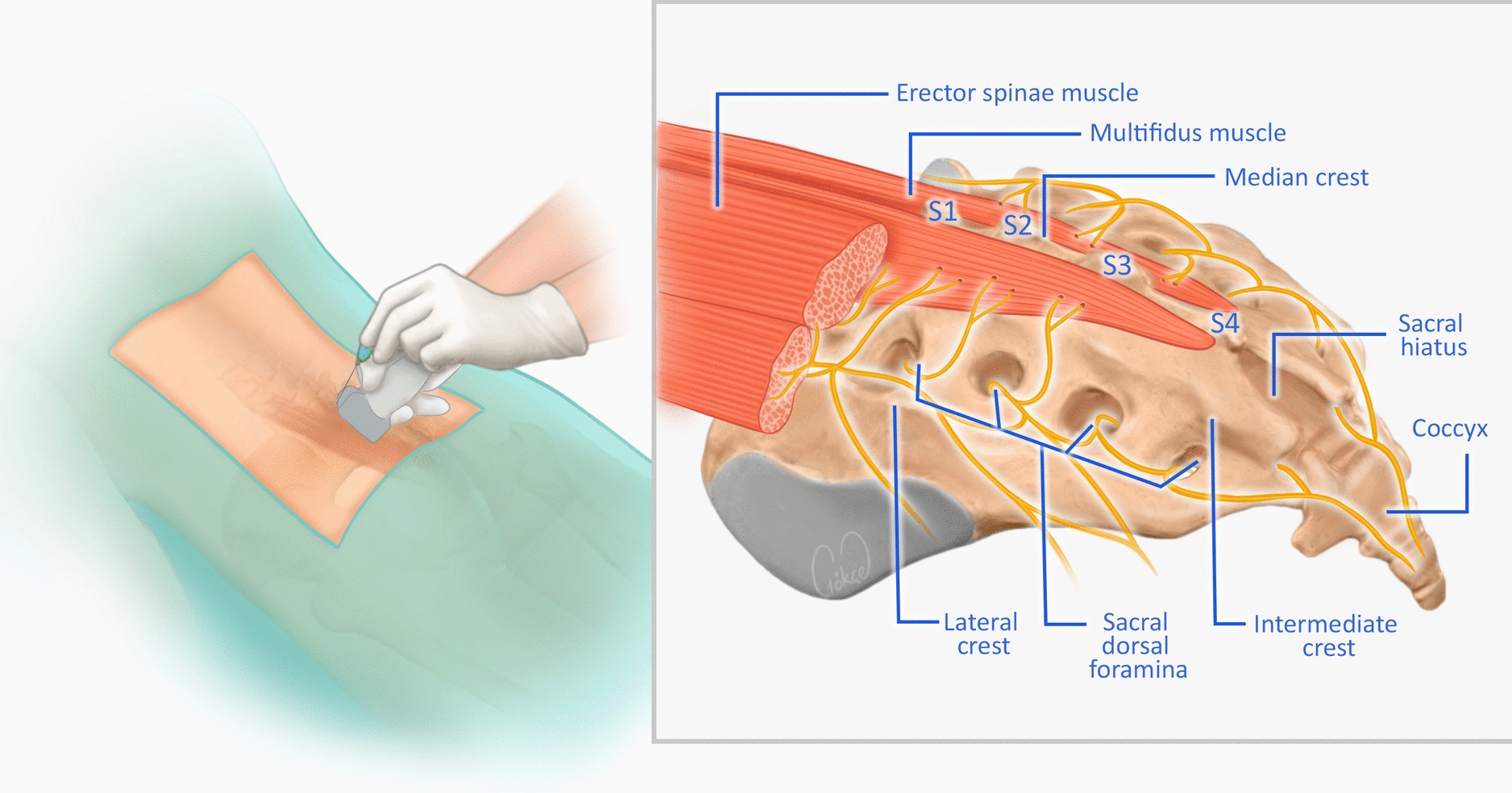
ProcedureAfter proper patient identification, obtaining written informed consent, and initiation of standard cardiopulmonary monitoring, the patient is placed in the supine position on the procedure table, allowing the physician to easily access and visualize the ilioinguinal nerve. The lower abdomen, iliac crest, and groin area on the affected side are prepared with three rounds of 2% chlorhexidine solution in 70% isopropyl alcohol and sterile draping. The skin and subcutaneous tissues 2 cm medial and inferior to the ASIS are anesthetized with 1–2 mL of 1% lidocaine using a 25-gauge needle to numb the skin before needle insertion [14]. A high-frequency (7–11 MHz) linear array ultrasound transducer is sheathed in sterile plastic and aligned in an oblique plane over the bony prominence of the patient's ASIS to the umbilicus (Fig. 2A) [30]. The probe is then slowly swept superiorly and inferiorly over the ilioinguinal canal while keeping the bony iliac crest visible in the lateral part of the image until the IIN is visualized in the fascial plane between the internal oblique and transversus abdominis muscles, often appearing as part of a bundle with the iliohypogastric nerve and the deep circumflex iliac artery (Fig. 2B) [30, 33]. The nerve is typically visualized as a small hypoechoic oval structure in short-axis transverse ultrasound views and as a hypoechoic linear structure when viewed in the long-axis longitudinal plane [30]. Under ultrasound guidance, a disposable radiofrequency cannula, 18–22-gauge, 100–150 mm in length, with a 5 or 10 mm active tip, is then advanced into the fascial space between the internal oblique and transversus abdominus muscles, where the IIN runs. The cannula is advanced using an in-plane ultrasound approach, which allows continuous visualization of the needle tip as it enters the fascial plane. A brief long-axis view may be used when needed to confirm cannula alignment before returning to the short-axis view for lesioning.
Fig. 2 The alt text for this image may have been generated using AI.
The alt text for this image may have been generated using AI.Adapted from Waldman and Willis, A Simplified Approach to Ultrasound-Guided Ilioinguinal Nerve Block, OAText, published under the Creative Commons Attribution 4.0 International License (CC-BY 4.0). No changes were made other than cropping and overlaying the images. License information: https://creativecommons.org/licenses/by/4.0/
Ultrasound-guided identification of the ilioinguinal nerve (IIN) and surrounding anatomical structures. A Patient positioning and ultrasound probe placement. B The IIN travels with the iliohypogastric nerve between the internal oblique and transverse abdominis muscles [30].
To ensure accurate placement of the needle within the correct pain-signaling nerves while avoiding damage to motor nerves, sensory stimulation at 50 Hz is performed to reproduce the sensation corresponding to the patient’s primary pain complaint. Suppose the sensory testing is negative for reproduction of paresthesia. In that case, the cannula tip is repositioned, and sensory testing is repeated until the patient experiences reproduction of pain or sensation in the area of symptoms. After positive sensory testing, motor stimulation is performed at 2 Hz up to 2 V and is considered appropriate if there is no motor response distal to the needle insertion site. A diagnostic nerve block with 2% lidocaine or 0.25% bupivacaine with or without a steroid is typically administered before radiofrequency lesioning to ensure short-term pain relief.
RFA is then performed using continuous radiofrequency (lesion) mode. For consistency, continuous RFA is performed at 80 °C for 60–90 s, which reflects established RFA technique recommendations and aligns with published procedural parameters. This conventional technique delivers sustained energy at 80 °C for 60–90 s to create a thermal lesion [12]. If the patient received complete pain relief for the initial round of RFA, the needle is removed, and a sterile dressing is applied to the insertion site. However, if pain persists, the needle is repositioned a few millimeters medially or inferiorly from the initial target to identify the iliohypogastric and genitofemoral nerves, as anatomical variation and overlap of these nerves can contribute to the sensation of pain [34]. After another sensory and motor testing round, RFA lesioning is performed again. Needles are removed after the procedure, and the skin is cleaned and prepared with a sterile dressing. Patients remain in the recovery room for 15 min after the procedure, during which a nurse monitors their vitals and checks for any adverse events, including temporary pain, swelling, numbness, bleeding, or neuritis at the needle insertion site, as well as signs of possible infection and fever. Patients are educated on returning if symptoms worsen or if signs of infection develop, scheduled for a follow-up appointment approximately 6–8 weeks after the procedure, and discharged on the same day as the procedure.
Dr. Alaa Abd-Elsayed has expanded upon the use of RFA by investigating the application of cooled RFA techniques. Although the procedural framework parallels that of conventional thermal RFA, the cooled method employs 17-gauge, 100-mm radiofrequency probes with 4-mm active tips to deliver lesions at 80 °C for approximately 2 min and 30 s, demonstrating consistent and reproducible efficacy [11, 17]. Considering the anatomical variability of the ilioinguinal nerve, needle placement should be guided by the patient’s reported area of pain, with sensory testing performed before ablation to confirm accurate targeting.
Alternatively, other providers have explored the use of pulsed radiofrequency (RF) as a therapeutic modality for ilioinguinal neuralgia. This technique utilizes a 27-gauge needle to deliver short, intermittent bursts of electrical energy, allowing the nerve to cool between pulses. For this procedure, the IIN is treated with 20 ms radiofrequency pulses at a frequency of 2 Hz for 120 s at a maximum temperature of 42 °C [15, 34]. Additionally, other providers have adapted this procedure using fluoroscopic guidance instead of ultrasound techniques for proper needle placement. Although the IIN is more easily identified on ultrasound, it can be visualized under fluoroscopic guidance by first locating the ASIS and iliac crest and then placing the needle 0.5–1.0 cm medial to the ASIS. The needle is directed slightly inferomedially toward the expected course of the nerve, advanced until it contacts bone (the ilium), then retracted 1-2 mm to reach the fascial plane. While fluoroscopy can be used as an alternative to ultrasound, it is instead often used in conjunction with ultrasound to confirm needle placement before RFA. However, there is a lack of evidence in the literature supporting the use of fluoroscopy to identify the IIN.
Key Technical TipsImportant technical considerations include maintaining continuous visualization of the cannula tip by using an in-plane ultrasound approach whenever possible. Identifying the deep circumflex iliac artery with color Doppler early in scanning helps to confirm the correct fascial layer containing the ilioinguinal nerve. Sensory stimulation should be performed before final cannula advancement, since adjusting the needle by only a few millimeters can significantly improve targeting when there is anatomical variability. When the nerve is difficult to visualize, sweeping cranially and caudally from the ASIS improves the likelihood of locating the correct fascial plane. Briefly switching to a long-axis view may also help to confirm the needle path before returning to the short-axis view for lesioning.
Common PitfallsSeveral common challenges may affect procedural success. The iliohypogastric nerve may be mistaken for the ilioinguinal nerve because they frequently travel together in the same fascial plane; therefore, sensory stimulation is essential to ensure accurate targeting. Omitting motor testing increases the risk of inadvertently affecting nearby motor branches, including the genitofemoral nerve. Lesioning too superficially can result in incomplete ablation, especially in patients with increased soft tissue depth. Scanning too narrow an area near the ASIS may miss variant nerve branches, so a broader cranial-caudal sweep is recommended. Additionally, relying solely on fluoroscopy introduces limitations because the nerve itself cannot be visualized, which increases the chance of suboptimal lesion placement.
These recommendations, which consist of a standardized sequence of sterile preparation, ultrasound-guided needle placement, sensory and motor testing, diagnostic block, and continuous RFA in lesion mode, consistently yield significant and sustained pain relief in patients with ilioinguinal neuralgia.
Comments (0)