
Remember me
The block may be performed with the patient in either the prone or lateral decubitus position. Prone positioning generally offers more stable access and facilitates bilateral application, whereas the lateral decubitus position may be preferred for patients with respiratory limitations or intolerance to prone positioning.
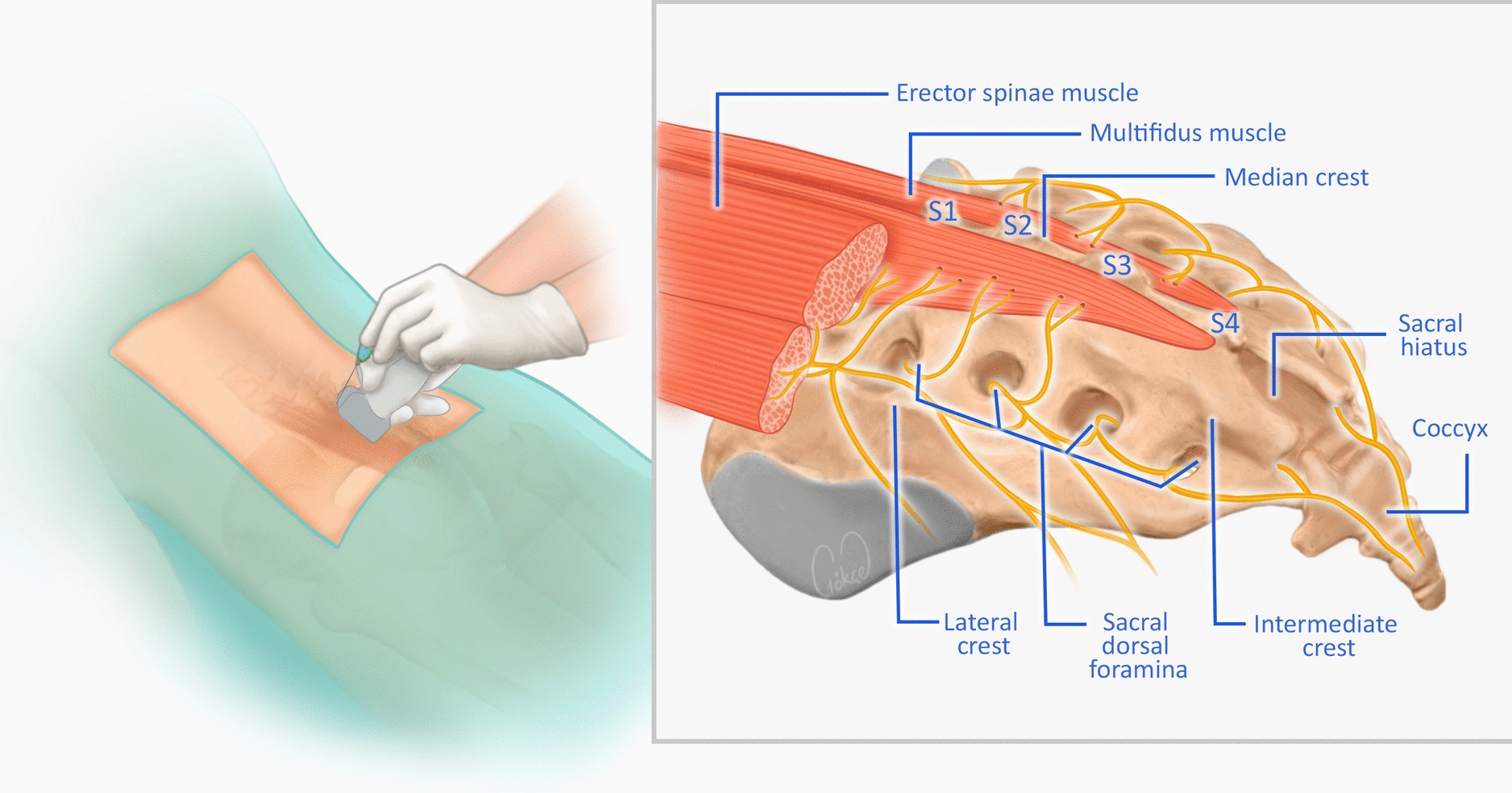
SonoanatomyThe S2 level can be reliably approximated by a line connecting the posterior superior iliac spine. It may be identified by palpating the posterior sacral landmarks or locating the sacral hiatus on a longitudinal midline ultrasound view and counting cranially. Once S2 is confirmed, scanning is initiated using a high-frequency linear transducer to visualize the sacral bony contours and fascial layers overlying the erector spinae–multifidus complex. In patients with obesity or limited image resolution, a low-frequency curvilinear probe may be required to improve penetration and overall image quality. The paramedian S-ESP block can be performed using either a transverse or longitudinal imaging plane. The choice of approach depends on the operator’s preference, patient habitus, and the desired needle trajectory; however, both techniques aim to deposit local anesthetic deep to the erector spinae–multifidus fascial plane at the S2 level in the line of the intermediate sacral crest.
Transverse ViewAfter confirming the S2 level, the ultrasound transducer is positioned transversely over the median sacral crest, which appears as a continuous hyperechoic line with posterior acoustic shadowing. From this point, the probe is moved laterally until the erector spinae aponeurosis is visible as a superficial hyperechoic fascial layer overlying the hypoechoic sacral multifidus muscle. Deep to the multifidus, the intermediate sacral crest is identified as a distinct hyperechoic bony ridge with a characteristic acoustic shadow. This structure serves as a key sonographic landmark for the needle orientation. Lateral to the intermediate crest, the sacral foramina can be recognized as focal interruptions in the cortical outline of the sacrum, appearing as small hypoechoic defects. Although the technique was originally described at the S2 level, the same sonographic principles and landmarks can be applied at other sacral levels, according to clinical indications.
Transverse In-Plane ApproachWith the transducer in the transverse orientation, the needle is advanced in-plane, most commonly from lateral to medial, although a medial-to-lateral trajectory is also feasible depending on ergonomics. The needle is advanced until gentle contact with the dorsal bony surface of the intermediate sacral crest is felt and observed sonographically [1]. The injection is performed medial to the sacral foramina.
Longitudinal Parasagittal ViewAlternatively, the target region can be identified using a longitudinal probe orientation. The transducer is first placed in the midline to visualize the sacral hiatus and confirm the S2 level. The probe is then shifted several centimeters laterally until the intermediate sacral crest comes into view. In this plane, the erector spinae aponeurosis appears superficially as a hyperechoic fascial layer, with the sacral multifidus muscle lying hypoechoic beneath it and the intermediate sacral crest forming a bright bony ridge deep to the multifidus. An alternative method is to begin at the lumbar level by identifying the transverse processes and then sliding the probe caudally toward the sacrum until the intermediate sacral crest is reached.
Parasagittal In-Plane ApproachWhen the transducer is positioned in a parasagittal orientation, the needle may be advanced cranio-caudally or caudo-cranially, depending on the operator’s preference. As in the transverse technique, the needle is guided until it reaches the bony surface of the intermediate sacral crest, maintaining the needle tip deep to the sacral multifidus and superficial to the sacral dorsal surface. The same precautions to avoid the sacral foramina apply in this view.
Out-of-Plane ApproachAn out-of-plane approach may also be used in both the transverse and longitudinal parasagittal views, provided that the needle tip is visualized clearly at all times. The needle should be advanced slowly with frequent adjustments to maintain visualization, ensure accurate placement within the intended potential plane, and avoid unintended entry into the sacral foramina (Fig. 3).
Fig. 3 The alt text for this image may have been generated using AI.
The alt text for this image may have been generated using AI.Ultrasound-guided S-ESP block using the paramedian approach. A Probe and needle positioning over the sacral region. B Corresponding ultrasound image showing the needle trajectory and injectate spread (blue line)
Injection Technique (General Considerations)In both ultrasound-guided approaches, the injection is directed into the potential space located deep to the sacral multifidus and superficial to the dorsal sacral surface at the level of the intermediate sacral crest. The deposition of local anesthetic within this plane facilitates longitudinal (cranio-caudal) spread along the sacral lamina, contributing to effective multilevel analgesia. Throughout the procedure, continuous visualization of the needle tip is essential to ensure accurate placement and to minimize the risk of inadvertent intramuscular or intraforaminal injection. For midline procedures, such as pilonidal sinus surgery, the block should be performed bilaterally to ensure symmetrical coverage of the sacral dermatomes.
Comments (0)