Participants with chronic, intractable trunk and/or limb pain were enrolled in the prospective, multicenter ECAP Study [23]. The ECAP Study (NCT04319887, registered 24 March 2020 on ClinicalTrials.gov, first enrollment 29 October 2020) was conducted in accordance with the United States Food and Drug Administration (FDA) regulatory requirements, good clinical practice (GCP, per ISO 14155), Western Institutional Review Board approval (WIRB ID 1290548), and the Declaration of Helsinki guided ethical principles. All patients provided written informed consent prior to participation in the study. This real-world study included patients with a wide range of pain locations and indications, including chronic back and leg pain and upper limb pain (Table 1). Each patient underwent a temporary SCS trial using an external stimulator capable of ECAP-controlled CL-SCS (Evoke® System, Saluda Medical, Bloomington, MN, USA) connected to one or two percutaneous Evoke® leads (12 contacts, all capable of stimulation and ECAP measurement) placed in the dorsal epidural space of the spinal canal. Patients who achieved a successful trial were eligible for permanent implantation of the Evoke System. As a real-world, pragmatic study, the duration of the temporary trial phase could vary by physician, clinic, region and insurance requirements, and therefore, could range from hours up to 30 days.
Table 1 Baseline characteristics, pain regions, and etiologyAt a single center in the ECAP Study, we evaluated outcomes during the trial phase and the permanent implant phase up to 12 months for patients who underwent an evaluation for a shortened trial immediately following the trial procedure (day 0 evaluation). Similar to the previous analysis [16], the day 0 evaluation included assessment of PPR (pain test), functional improvement (function test), and willingness to proceed to a permanent implant (willingness test). On the day of the trial procedure, patients were informed preoperatively that if they met the day 0 evaluation success criteria—passing the pain and function tests and responding “Yes” to the willingness test—after successful configuration of ECAP-controlled CL-SCS, the decision to proceed with permanent implantation could be made immediately, and their trial system implant could be removed the same day (day 0 trial). When this occurred, the day 0 visit was also the patient’s EOT visit. Alternatively, patients had the option to continue with a traditional trial. Peri-procedural sedation and analgesic use were per standard institutional protocol and not specifically controlled as part of this analysis.
Prior to offering a day 0 trial, patients were required to have insurance coverage that did not specify a mandated trial duration. No additional eligibility or exclusion criteria were applied beyond those specified for participation in the ECAP Study [23]. Day 0 evaluations were conducted over a contiguous period of time spanning August 2021 to November 2022.
The day 0 trial approach contrasts with “on-table” trials, where pain coverage and relief are assessed intraoperatively while the patient is positioned for surgery under restricted mobility, partial sedation, and often additional analgesic medication [6]. In comparison, the day 0 evaluation occurs post-implantation and programming of the trial system, once the patient has recovered from the lead insertion procedure and resumed unrestricted mobility.
Baseline Characteristics and Patient-Reported Outcomes
Baseline characteristics (age, body mass index (BMI), weight, height, and gender), primary pain regions, and etiology for patients were summarized. The patient-reported outcomes evaluated included Visual Analogue Scale (VAS) percent reduction for the primary area of pain at baseline (overall VAS), 30%, 50%, and 80% responder rates for overall VAS, Pain Impact Score (PIS), satisfaction with pain relief and therapy, Patient Global Impression of Change (PGIC) [23], and a holistic score reflecting the overall clinical benefit to patients [24]. The PIS is derived from the pain intensity, physical function, and pain interference subdomains of the Patient-Reported Outcomes Measurement Information System profile (PROMIS-29v2.1 [25]) and ranges from 8 (no pain impact) to 50 (highest pain impact), with a minimal clinically important difference (MCID) of 3 points [26]. The validated holistic cumulative responder score is calculated as the total number of MCIDs across seven domains of the PROMIS-29 questionnaire that were impaired at baseline, which include physical function, anxiety, depression, fatigue, sleep disturbance, social activities, and pain intensity [27, 28]. Appropriate approval for use was obtained for the PROMIS-29 questionnaire.
Neural Metrics
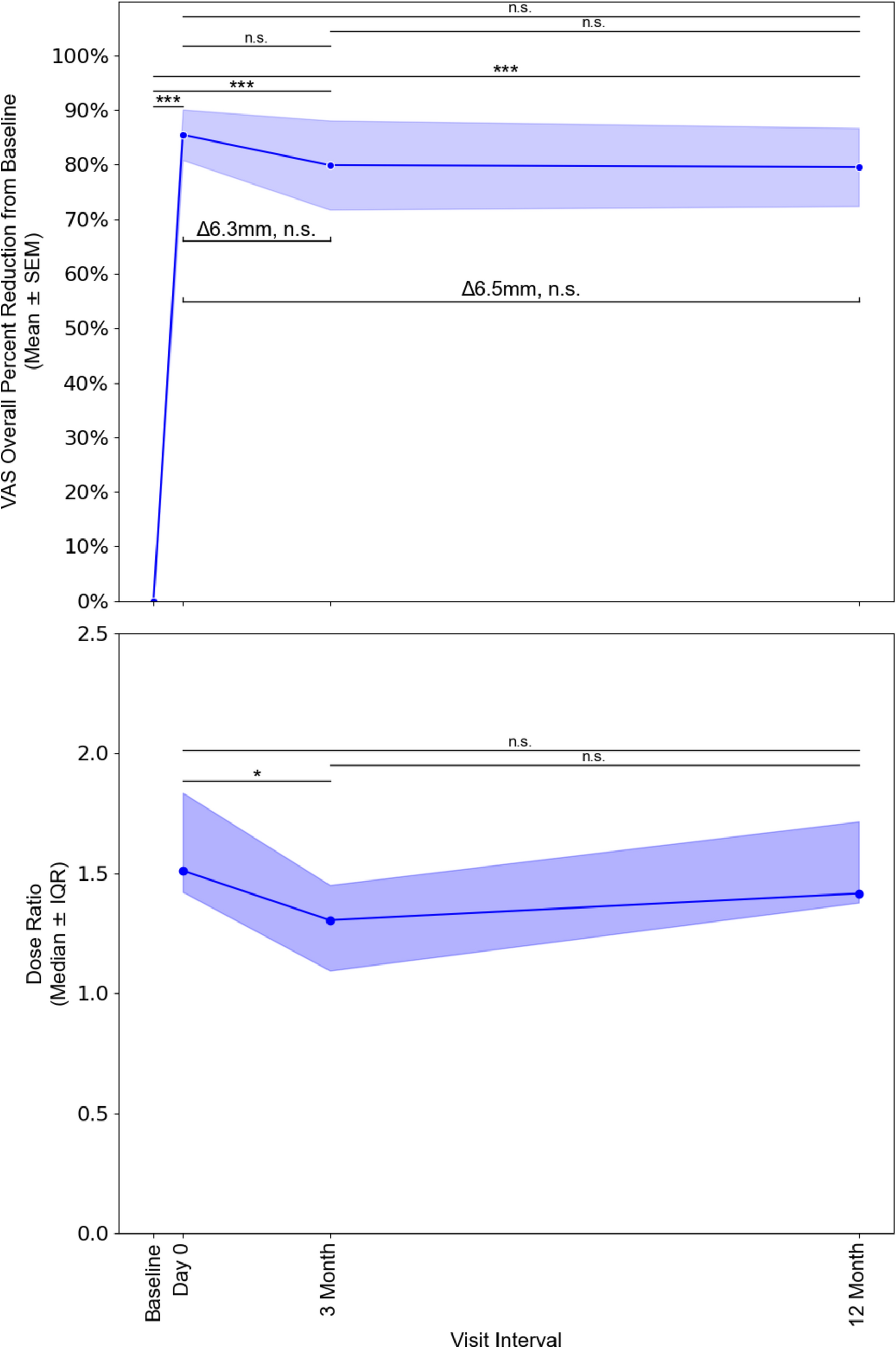
Data were collected on activation plots, median ECAP level at which the patient experienced stimulation (ECAP dose), ECAP dose level with respect to ECAP threshold (dose ratio), stimuli above ECAP threshold (therapy utilization), accuracy of the feedback loop (dose accuracy), and the percent of time the stimulator was used during each analysis period in the permanent implant phase (system utilization) [14,15,16, 29,30,31]. Dose ratio was calculated based on each patient’s preferred ECAP dose relative to their ECAP threshold, with a dose ratio of 1.0 representing therapy at ECAP threshold, and dose ratios of 1.2–1.6 associated with maximal pain relief [14, 15]. Dose accuracy was calculated as the root mean square error (RMSE) of measured ECAP amplitudes versus the target ECAP amplitude set on the patient’s Evoke SCS system. Therapy utilization was calculated as the percent of stimuli that were above ECAP threshold [14].
End of Trial Neural Metrics
Since patients experiencing a day 0 trial did not have out-of-clinic logs spanning several days at EOT due to their leads being pulled on the same day as the trial implant, system utilization at EOT is not applicable. Other neural panel metrics (therapy utilization, dose ratio, ECAP dose, and dose accuracy) were calculated using high-resolution ECAP recordings obtained during the in-clinic posture evaluation used to assess function improvement, similar to methods used previously [16].
Permanent Phase Neural Metrics
Permanent phase neural metrics were calculated using the out-of-clinic device logs following methods described previously [14, 29,30,31]. Metrics were calculated based on patient usage during the 1-week period leading up to the 3- and 12-month visits.
Statistical Analysis
Patient-reported outcomes are summarized as means with standard deviation (SD). Changes in VAS and PIS outcome data were tested for significance relative to baseline and across follow-up intervals (day 0 vs. 3 months, day 0 vs. 12 months, and 3 months vs. 12 months) using paired t-tests. Neural metrics are presented as medians and interquartile ranges (IQR), and the differences between intervals were assessed using the Wilcoxon signed-rank test. Statistical analyses were performed in Python v3.10 using the scipy and statsmodels packages with statistical significance defined at the 5% level.

Comments (0)