
Remember me
This study was approved by the Medical Ethics Committee of the Affiliated LiHuiLi Hospital of Ningbo University, China (KY2023PJ297), and the protocol was registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn, ChiCTR2400080942) (prospectively registered). The initial registration date was 19 February 2024. This research was conducted in compliance with the ethical principles outlined in the Helsinki Declaration (1964 and later amendments). The methodology and findings are reported following the guidelines of the Consolidated Standards of Reporting Trials (CONSORT) statement. Written informed consent was obtained from all patients or legal representatives. The trial ran from February 2024 to July 2024.
The inclusion criteria included the following: aged between 18 and 70 years, American Society of Anesthesiologists (ASA) I–III, and scheduled for laparoscopic radical or partial nephrectomy. The exclusion criteria included the following: serious cardiopulmonary disease, history of central nervous system disorders and/or peripheral nerve injuries, severe liver or renal insufficiency, coagulopathy, long-term use of analgesic drugs (including opioid use) or a history of chronic pain syndromes, inability to communicate or cooperate, and allergic to LAs.
Grouping AdjustmentThe initial study protocol registered with the Chinese Clinical Trial Registry (ChiCTR2400080942) outlined three groups: a patient-controlled intravenous analgesia (PCIA) control group, an ultrasound-guided QLB (U-QLB) group, and a laparoscopic-assisted QLB (L-QLB) group. However, during the final ethical and protocol review prior to trial initiation, the Medical Ethics Committee and the research team concurred that a control group receiving only PCIA without regional nerve block, within the current standard of care emphasizing multimodal analgesia, could expose participants to a higher risk of postoperative acute pain. This was deemed inconsistent with ethical principles. To prioritize participant safety and rights, the decision was made before enrolling any patients to omit the control group. The study proceeded to compare only the two active intervention techniques (U-QLB and L-QLB).
This protocol amendment was reviewed and approved by the Medical Ethics Committee of the Affiliated LiHuiLi Hospital of Ningbo University (identifier: KY2023PJ297). All participants enrolled in this study were randomized and managed according to the revised two-group design.
Randomization and BlindingPatients were randomly allocated to one of two groups using a computer-generated random number sequence: the L-QLB group (group L) and the U-QLB group (group U). Allocation concealment was achieved via sequentially numbered, opaque, sealed envelopes that were prepared by an independent statistician not involved in patient recruitment or outcome assessment. On the day of surgery, after the induction of general anesthesia and according to the recruitment order, an experienced senior anesthesiologist (who was not involved in subsequent patient management or data collection) opened the envelope and prepared the study drug. This anesthesiologist then performed the U-QLB for patients in the U-QLB group. In contrast, patients in the L-QLB group received the L-QLB from a urological surgeon with over 10 years of experience in laparoscopic renal surgery who performed more than 50 laparoscopic nephrectomies annually. All patients, postoperative outcome assessors, and statisticians remained blinded to the group allocation throughout the study.
General Anesthesia and Study InterventionAll patients underwent standard monitoring, including a 5-lead electrocardiogram, pulse oxygen saturation, invasive arterial blood pressure, and bispectral index (BIS). Peripheral and central intravenous access were established. Both groups received general anesthesia. Anesthesia was induced intravenously (propofol 2 mg/kg, sufentanil 0.4 μg/kg, and rocuronium 0.8 mg/kg) following pre-oxygenation. Patients were then intubated and given an intravenous anesthesia (propofol 0.1–0.15 mg/kg/min and remifentanil 0.1–0.3 μg/kg/min) to maintain the BIS between 40 and 60. Rocuronium (20 mg) was administered intravenously as intermittent boluses to maintain muscle relaxation.
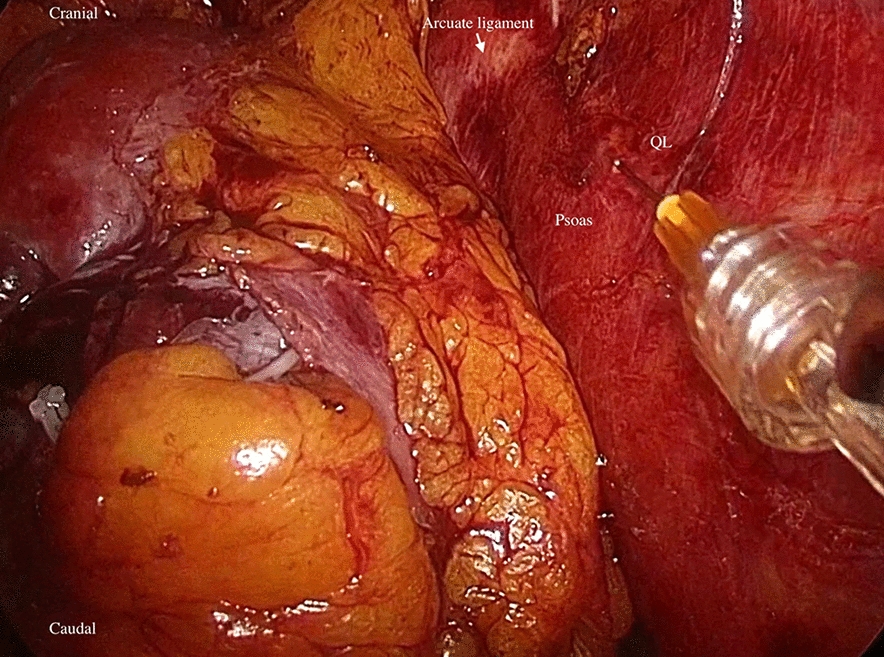
L-QLB was performed in the L group prior to surgical closure. Once the kidney was removed, the QL muscle with anterior layer of the thoracolumbar fascia (TLF) was clearly identified lateral to the psoas. An injection needle attached to an extension tube was directly inserted into the fascial plane between the QL and PM muscles under the direct visual guidance of laparoscopy, with a depth of approximately 0.5 cm under the TLF (Fig. 1). The needle tip position was verified by injecting 2 mL of normal saline to separate the fascial layers. A total of 30 mL of 0.25% ropivacaine was slowly administered.
Fig. 1 The alt text for this image may have been generated using AI.
The alt text for this image may have been generated using AI.Laparoscopic-assisted QLB. QL muscle seen lateral to the psoas muscle. QL quadratus lumborum
U-QLB was performed on patients in the U group immediately after skin closure in the operating room, prior to emergence from general anesthesia. The interval between the performance of L-QLB (performed prior to surgical closure) and U-QLB (performed immediately after skin closure) was approximately 10 min. A curvilinear probe (2–5 HZ, Edge, Sonosite, Seattle, USA) was placed transversely between the 12th rib and iliac crest. After identifying the erector spinae (ES), QL, and PM muscles, a 22-gauge, 80-mm needle was advanced to the anterior part of the QL muscle. Its tip was then positioned between the QL and PM muscles using the in-plane technique (Fig. 2). After confirming the site via hydrodissection, 30 mL of 0.25% ropivacaine was slowly injected. No additional port-site or wound infiltration analgesia was performed in both groups.
Fig. 2 The alt text for this image may have been generated using AI.
The alt text for this image may have been generated using AI.Image of ultrasound guided QLB. LA spread between QL and PM muscles. The arrow indicates the trajectory of the needle. QL quadratus lumborum, PM psoas major, ES erector spinae, LA local anesthetic
Postoperative AnalgesiaAll subjects received intravenous sufentanil (0.2 μg/kg) and tropisetron (2 mg) 10 min before the end of the surgery. After surgery, a patient-controlled intravenous analgesia (PCIA) pump containing sufentanil (2 μg/kg) and tropisetron (0.15 mg/kg) in 100 mL of normal saline was initiated with the following settings: a 2 mL/h background infusion, a 0.5 mL demand bolus, and a 15-min lockout period.
Following surgery, all patients received 40 mg of intravenous (IV) parecoxib sodium every 12 h. If patients expressed breakthrough pain [visual analog scale (VAS) scores ≥ 4], 100 mg tramadol was administered intramuscularly for rescue analgesia.
No patients in either group received any adjunct regional analgesia techniques or non-protocol opioid medications beyond the standardized perioperative analgesic regimen.
Evaluation of Sensory BlockPatients were assessed for sensory blockade by an anesthesiologist blinded to this study, 2 h after surgery. The extent of cutaneous sensory blockade was evaluated along the midaxillary line on the surgical side. Cold sensation was evaluated using a cold alcohol swab, with sensory blockade defined as reduced or absent sensation [10]. Intact sensations on the contralateral abdominal walls were used for comparisons.
OutcomesThe primary outcome was cumulative sufentanil consumption within the first 24 h after surgery.
Secondary outcomes included the procedural time of QLB; the dermatomes of sensory block 2 h after surgery; resting and coughing VAS pain scores at 6, 12, 24, and 48 h postoperatively; rescue analgesia rate during the 0–48 h period after surgery; patient satisfaction with pain relief at 24 h post-surgery determined via a Likert scale (1 = very dissatisfied, 2 = dissatisfied, 3 = neutral, 4 = satisfied, and 5 = very satisfied); and adverse events, such as vascular puncture, LA systemic toxicity (LAST), postoperative nausea, vomiting, dizziness, and respiratory depression (defined as oxygen saturation < 90% or respiratory rate < 8 breaths per minute).
Postoperative pain was evaluated using the VAS, scored from 0 to 10, where 0 indicates no pain and 10 indicates excruciating pain. According to this scale, scores of 1–3 were classified as mild pain, 4–6 as moderate pain, and 7–9 as severe pain [11].
The procedural time for the L-QLB group was defined as the period from the needle holder’s entry into the posterior abdominal cavity to the completion of drug injection. For the U-QLB group, it was defined as the period from the placement of the ultrasound probe on the abdominal wall to the end of injection.
Statistical AnalysesThe sample size of this study was calculated using IBM SPSS Sample Power version 3.0. Our pilot study with ten patients showed that postoperative 24-h sufentanil consumption (μg mean ± standard deviation) was 27.9 ± 4.5 in the L-QLB group and 32.7 ± 5.3 in the U-QLB group, with a between-group difference of 4.8 μg, with a standard deviation of 5.0 (yielding an effect size, Cohen’s d, of 0.96). A sample size of 23 participants per group was required to provide 90% power at an alpha level of 0.05. A total of 30 patients in each group were recruited to account for potential dropouts and loss to follow-up.
Statistical analyses were conducted using SPSS V.24.0. The Kolmogorov–Smirnov test was used to evaluate normality. Continuous variables following a normal distribution are presented as means ± standard deviations (SD) and analyzed using the independent-samples Student’s t-test, while non-normally distributed ones are summarized as median (interquartile range, IQR) and analyzed via nonparametric tests (e.g., Mann–Whitney U test). Categorical variables are summarized as frequencies with percentages. A repeated-measures analysis of variance (ANOVA) was applied to evaluate differences between the two groups across multiple time points. For categorical variables, the Chi-squared (χ2) test or Fisher’s exact test was employed. A 95% confidence interval (CI) for mean differences (MD) (continuous variables) or relative risk (RR) (categorical variables) were calculated. Statistical significance was defined as a P-value below 0.05. To control for the risk of false positives due to multiple comparisons, a Bonferroni correction was applied to adjust the statistical significance threshold specifically for the post hoc comparisons of repeated-measures outcomes across different time points and for the group comparisons of secondary efficacy endpoints.
Comments (0)