To our knowledge, this randomized controlled trial is the first to assess the efficacy of taVNS for postoperative pain relief in patients undergoing gastrointestinal tumor surgery. Compared with control stimulation group, taVNS resulted in a significantly greater reduction in VAS pain scores from pre- to post-stimulation at 24 h postoperatively. In addition, taVNS was associated with lower rescue opioid requirements at 48 and 72 h postoperatively and more rapid recovery of gastrointestinal function, as indicated by an earlier time to first flatus. Collectively, these findings provide evidence supporting the feasibility and potential clinical value of taVNS as an adjunctive analgesic strategy during abdominal surgery.
Although a growing body of literature has demonstrated the analgesic benefits of taVNS in chronic pain conditions, its role in perioperative pain management remains unclear [17]. Findings from studies in other surgical contexts offer important context for our results. In a randomized trial involving patients undergoing perianal surgery, taVNS significantly reduced both VAS scores during the first postoperative dressing change and supplemental analgesic requirements [19]. In patients undergoing video-assisted thoracoscopic lobectomy, Zhang et al. observed that taVNS reduced acute postoperative pain, lowered the incidence of rebound pain, and decreased the 3-month prevalence of chronic postsurgical pain [20]. Similarly, a randomized controlled trial demonstrated that taVNS significantly reduces postoperative opioid consumption and lowers pain scores in patients undergoing arthroscopic shoulder surgery [21]. Additionally, Patel et al. observed a 19-mm reduction in VAS scores within 24 h of taVNS administration in patients with orthopedic trauma (compared to a 10-mm reduction with sham stimulation), with 78% of patients in the active group achieving clinically meaningful pain relief compared with only 38% in the sham group [22]. Notably, increased heart rate variability—reflecting enhanced parasympathetic activity—was observed only in the active taVNS group, suggesting effective vagal engagement and raising the possibility that autonomic modulation contributes to the analgesic effects. Overall, our findings are consistent with previous perioperative studies and further support the analgesic reliability of taVNS, particularly during the subacute postoperative phase.
The analgesic efficacy of taVNS is linked to stimulation duration and frequency. Animal studies have demonstrated that, compared to single-session stimulation, repetitive taVNS produces stronger and more sustained analgesia, characterized by gradually elevated pain thresholds and persistent attenuation of pain-related behaviors [23, 24]. Similarly, clinical trials have confirmed that taVNS raises pain thresholds in healthy volunteers, with efficacy increasing alongside the frequency of interventions [25, 26]. Our protocol incorporated both preoperative and postoperative sessions to maximize therapeutic benefit through repetitive stimulation [22]. Given the lack of a standardized control protocol for taVNS, we adopted a 1-Hz stimulation setting for the control stimulation group based on prior evidence [27, 28]. This parameter was chosen specifically to preserve the blinding of participants by mimicking the sensation of active stimulation.
Consistent with the observations of Zhang et al., our study found no significant difference in opioid consumption between groups during the first 24 postoperative hours [20]. However, cumulative MME was significantly lower in the taVNS group at both 24–48 and 48–72 h. This delayed analgesic effect may reflect a dose- or frequency-dependent activation of vagal pathways: repeated postoperative stimulation sessions may gradually enhance vagal tone and neuromodulation, leading to pronounced analgesia during the 24–72-h window, whereas a single preoperative session may not adequately alleviate immediate severe postoperative pain [22]. Furthermore, the anti-inflammatory and neuromodulatory effects of taVNS require a certain latency period to manifest [29], which may explain the lack of observable analgesia within 24 h and the progressive pain relief after 24 h.
The clinical benefits of taVNS across multiple endpoints—pain reduction, opioid sparing, and gastrointestinal recovery—have prompted exploration of its underlying mechanisms, which involve neuromodulation, autonomic regulation, and anti-inflammatory effects:
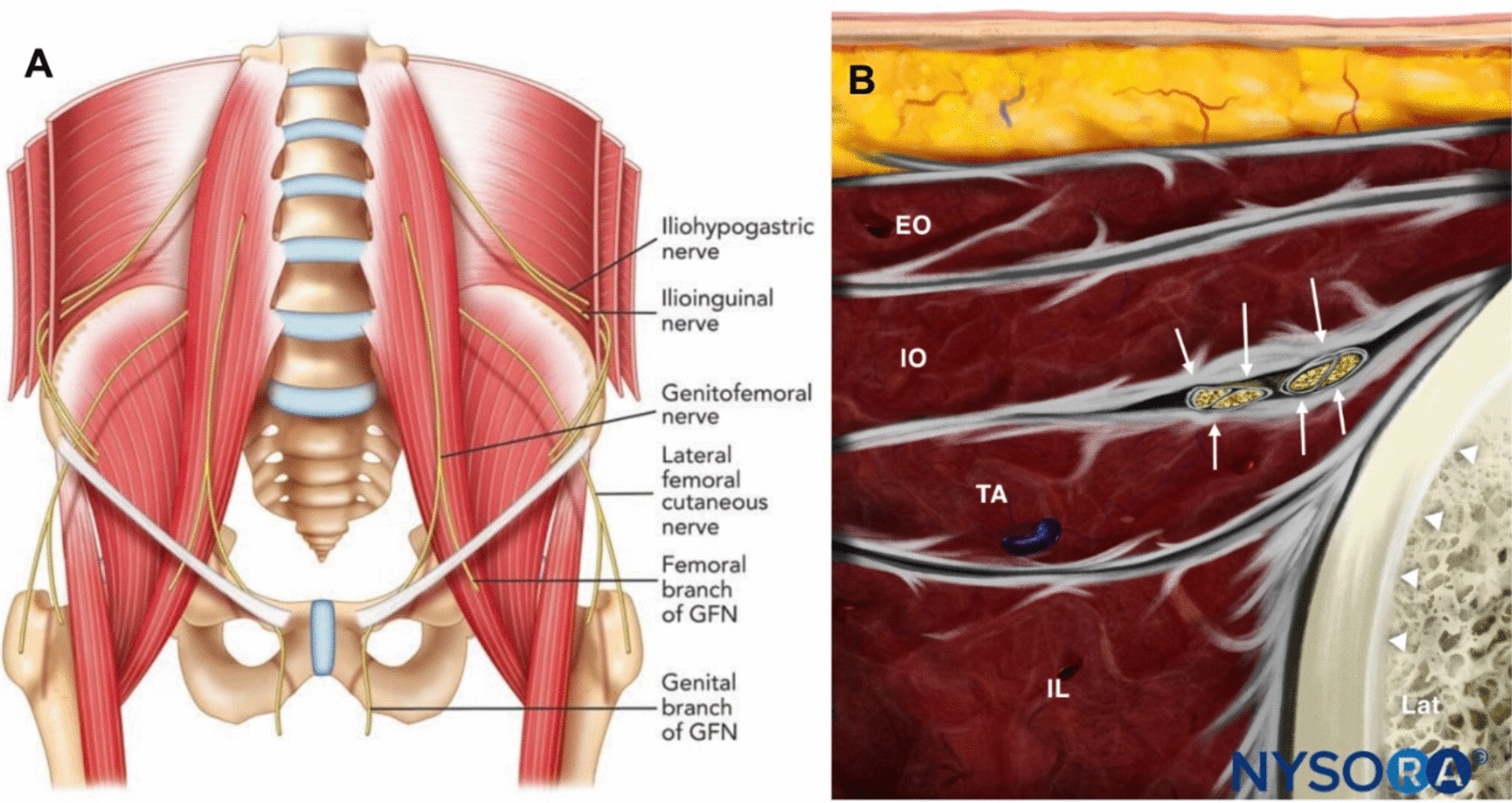
Neuromodulatory pathways: The auricular branch of the vagus nerve conveys afferent signals to the nucleus tractus solitarius in the medulla, the principal integration center for vagal input. The nucleus tractus solitarius then projects to key pain-modulatory centers, including the locus coeruleus, medullary reticular formation, and the raphe nuclei [30, 31]. TaVNS activates the locus coeruleus and dorsal raphe nucleus, core components of the descending inhibitory pathway. These nuclei modulate spinal nociceptive processing by releasing noradrenaline and serotonin, which act through spinal α2-adrenergic receptors and 5-hydroxytryptamine subtypes to attenuate pain transmission.
Autonomic regulation and anti-inflammatory effects: The vagus nerve plays a central role in parasympathetic control of cardiovascular and gastrointestinal function and mediates the cholinergic anti-inflammatory reflex. Vagal stimulation induces acetylcholine release, which binds to α7-nicotinic acetylcholine receptors on macrophages and suppresses pro-inflammatory cytokine production. By mitigating the postoperative inflammatory response, taVNS may reduce inflammation-related hyperalgesia and tissue edema. In patients with irritable bowel syndrome, a 4-week course of taVNS lowered circulating pro-inflammatory cytokines and enhanced vagal activity, and these physiological changes correlated with improvements in abdominal pain and bowel habits [32]. These mechanistic links provide a plausible explanation for the shorter time to first flatus observed in the taVNS group in our study.
Building on prior research, our study advances the application of taVNS in perioperative care in three key ways. First, it extends the use of taVNS to major abdominal procedures, such as gastrointestinal tumor surgery, thereby expanding the evidence base for its postoperative analgesic effects. Second, beyond pain intensity and opioid consumption, we examined gastrointestinal recovery and postoperative complications, confirming dual benefits in analgesia and functional recovery and linking these outcomes to autonomic modulation. Third, by situating taVNS within the framework of enhanced recovery after surgery (ERAS), we highlight its potential role as a nonpharmacological adjunct to support ERAS pathways and improve postoperative recovery quality.
Limitations and Future
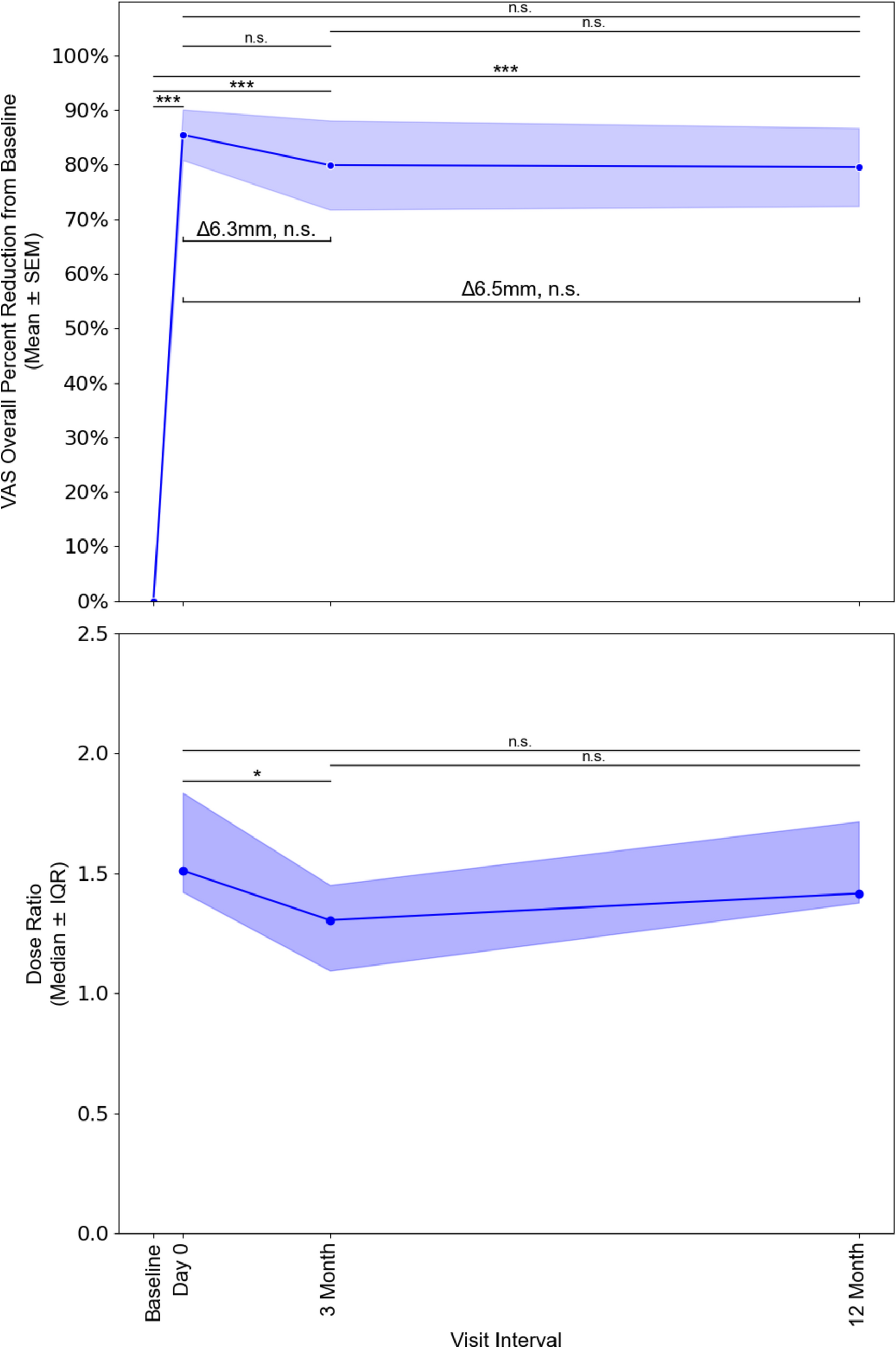
Although this study used a randomized controlled design, its generalizability and statistical power are limited by its single-center setting and moderate sample size. Larger multicenter trials are needed to improve the generalizability of conclusions and confirm the efficacy and safety of taVNS. In addition, this study enrolled only participants with a BMI < 30 kg/m2 to minimize the safety risks and potential confounding effects associated with obesity-related alterations in pain perception and opioid pharmacokinetics. This design limits the generalizability of our findings, warranting further research to evaluate the analgesic efficacy of taVNS in patients with obesity. Another limitation is the absence of regional anesthesia techniques in the analgesic regimen. However, considering that these techniques require specific expertise and ultrasound technology, our protocol’s reliance on PCIA better reflects real-world clinical practice, especially in resource-limited settings. Although pain reduction within the taVNS group exceeded the minimal clinically important difference (MCID), the intergroup difference of 7 mm fell below the 10-mm threshold, suggesting limited clinical significance under the current protocol. Given the cumulative analgesic nature of taVNS, future studies should prioritize optimizing stimulation paradigms and extending durations to fully enhance and validate its clinical value. Finally, the mechanistic understanding behind taVNS can further be deepened by assessing objective physiological measures such as heart rate variability as a reflection of real-time changes in vagal tone, along with laboratory findings, such as inflammatory biomarker.

Comments (0)